
Cardiology — MCQs

On this page
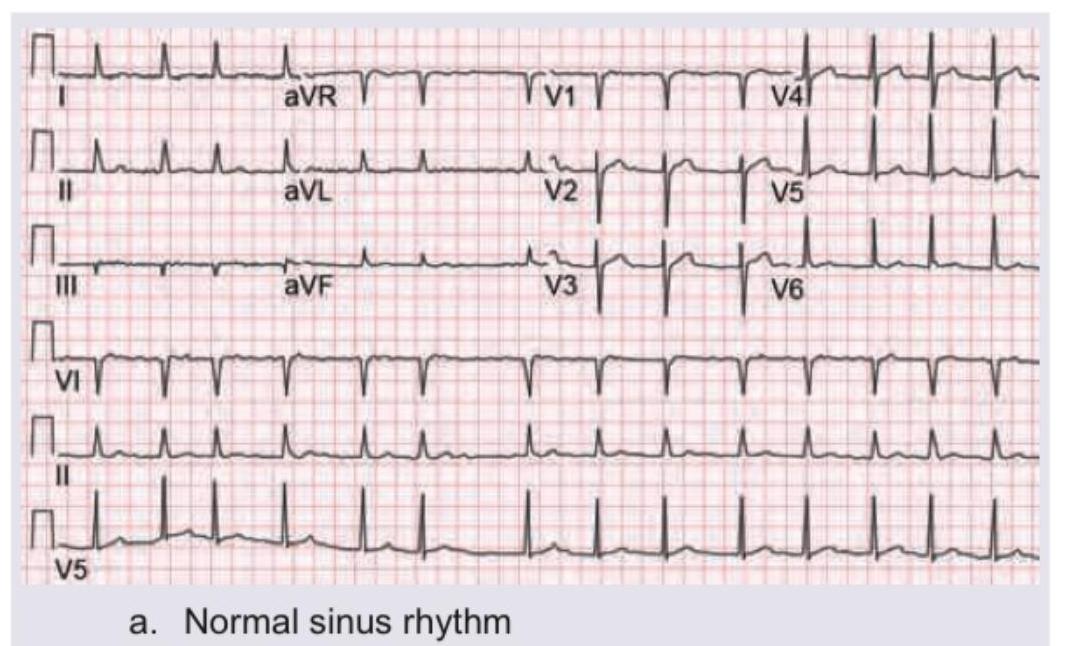
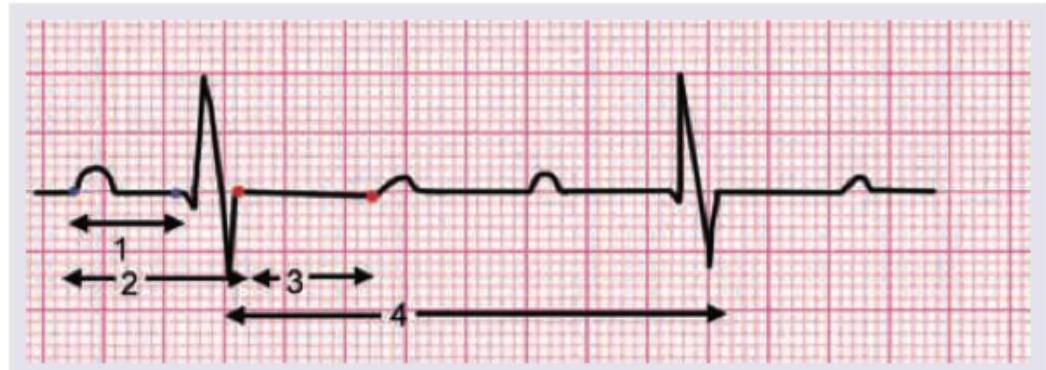
Identify the ECG finding shown below:
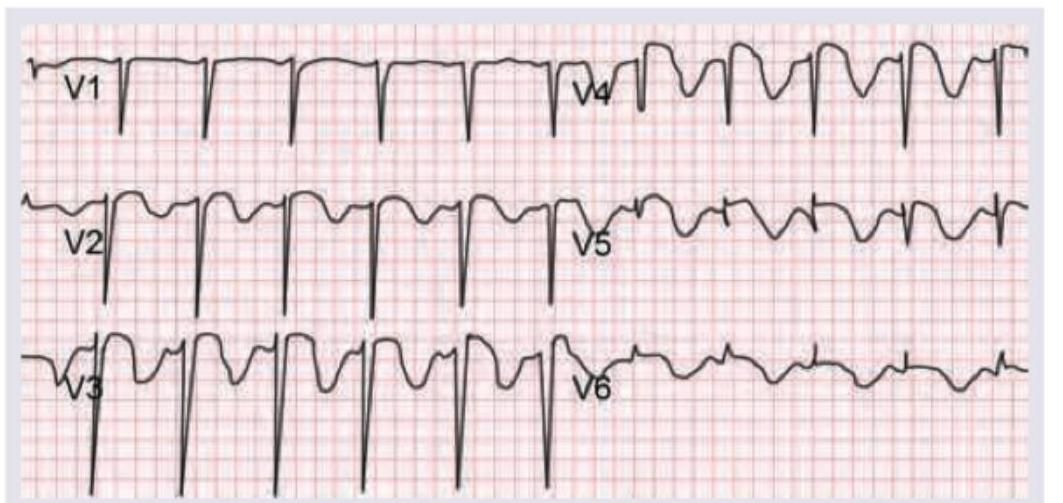
A 75-year-old male patient presents to the AIIMS emergency with retrosternal chest pain for 6 hours. The following ECG was done. What will be the primary management of the patient?
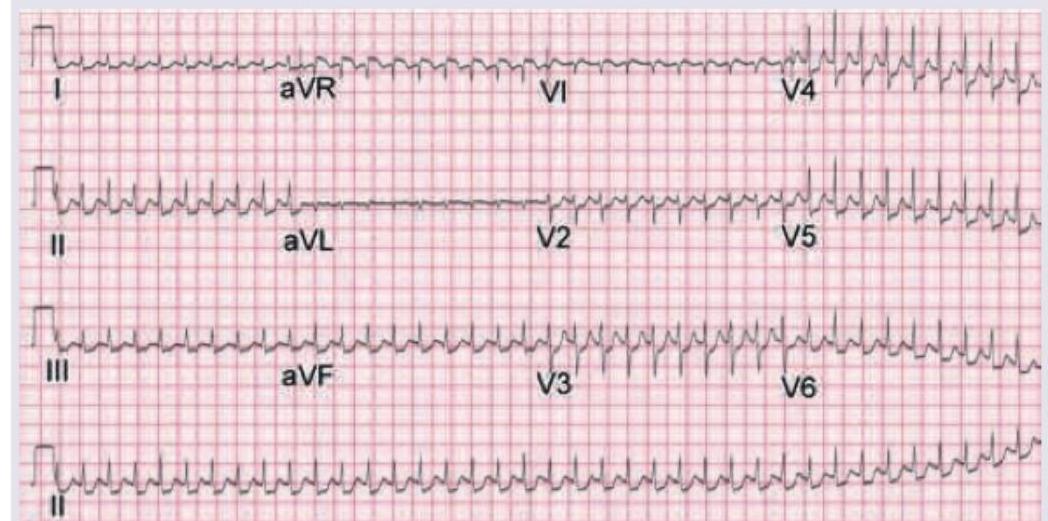
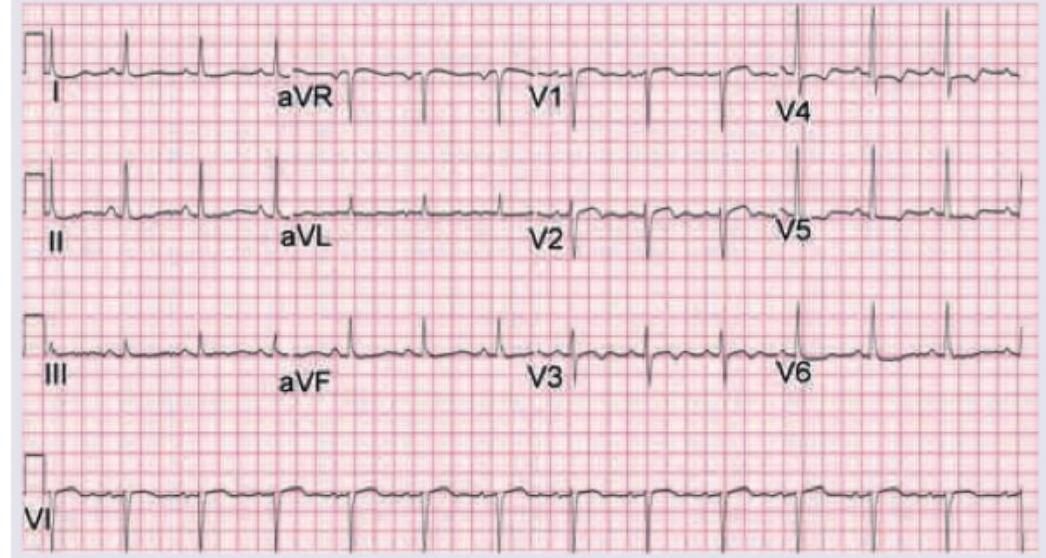
A 52-year-old male diabetic patient presents with palpitations to the AIIMS emergency. Urgent ECG was performed. What is the immediate next step in the management?
A 65-year-old elderly male has history of sweating and chest pain for last 24 hr with the following ECG. Which of the following is not given in managing the patient?
Identify the ECG given in the figure below.
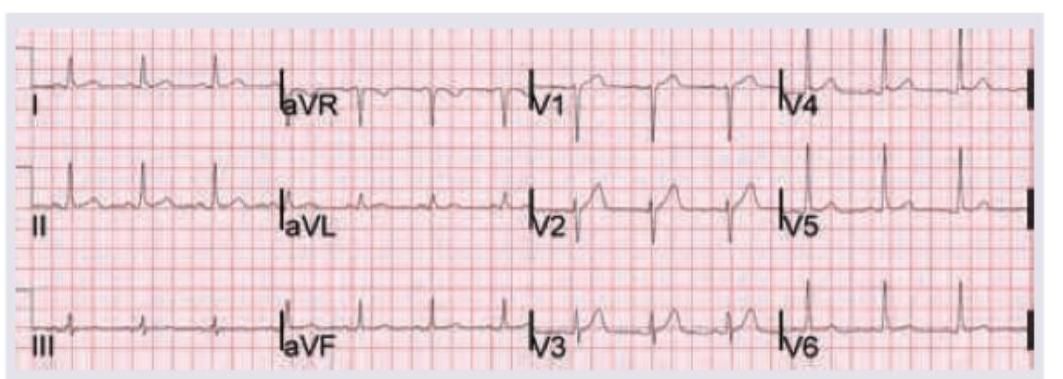
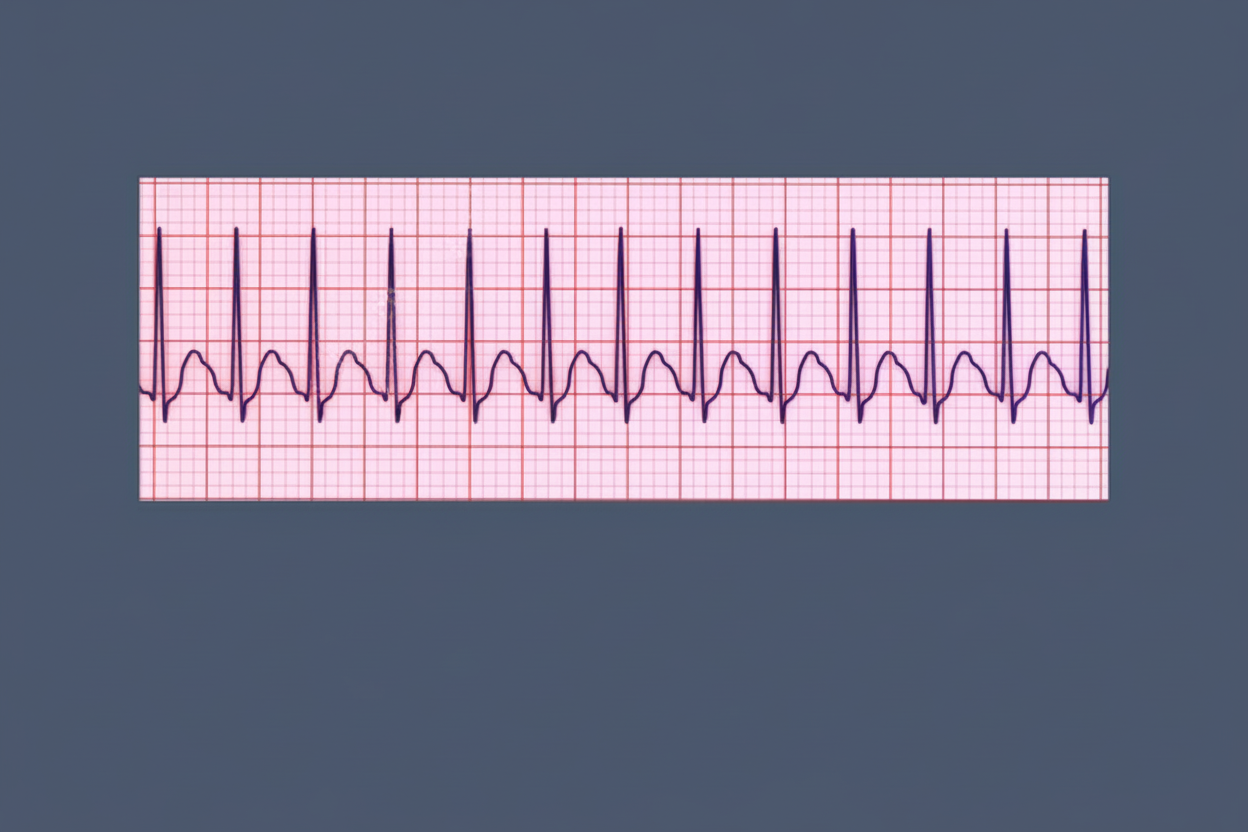
A 25-year-old woman presents with complaints of recurrent episodes of sudden onset palpitations. What does her ECG tracing show?
A 42-year-old male with poorly controlled diabetes presents with stuttering chest pain for up to 15 minutes at a time over 24 hours. He is pain-free at the time of this ECG. ECG shows:
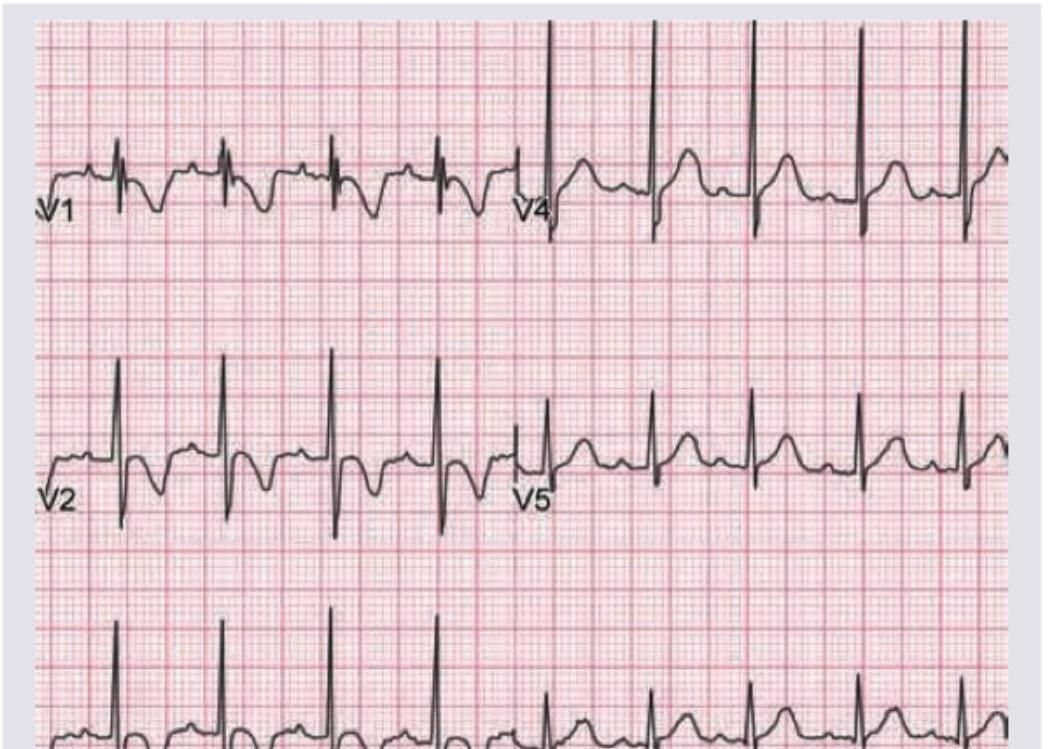
Which of the following finding is shown in the chest leads?
Corrected QT (QTc) is calculated by dividing QT/x. What is the value of x as per given ECG.
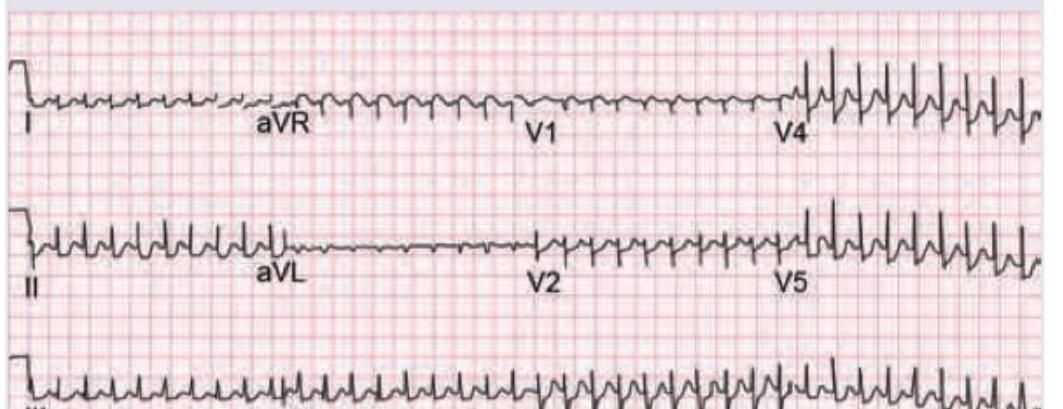
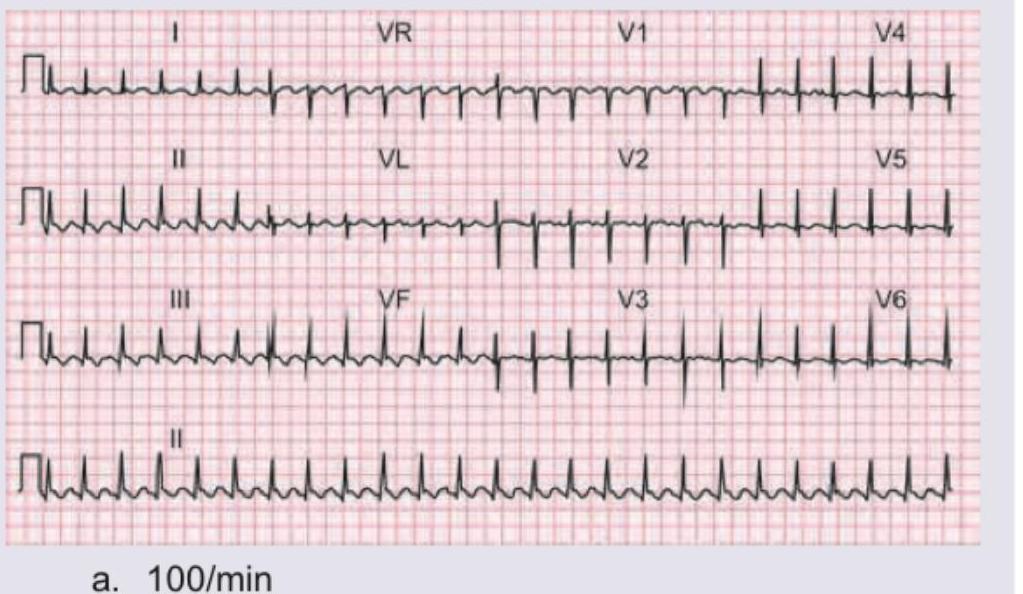
A 40-year-old man was admitted to the hospital emergency with sudden onset of the symptoms and signs of severe left ventricular failure. Calculate the atrial rate of the patient:
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app