
Cardiology — MCQs

On this page
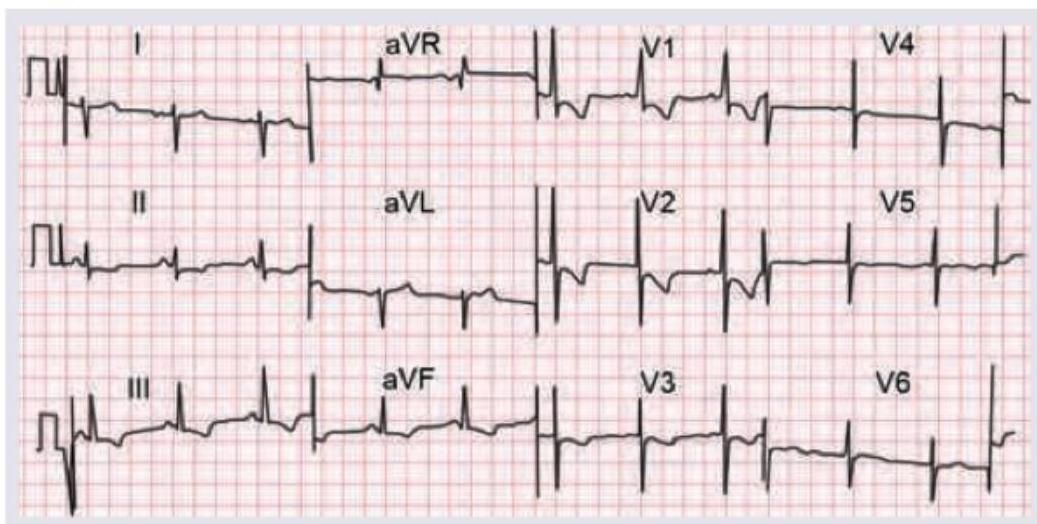
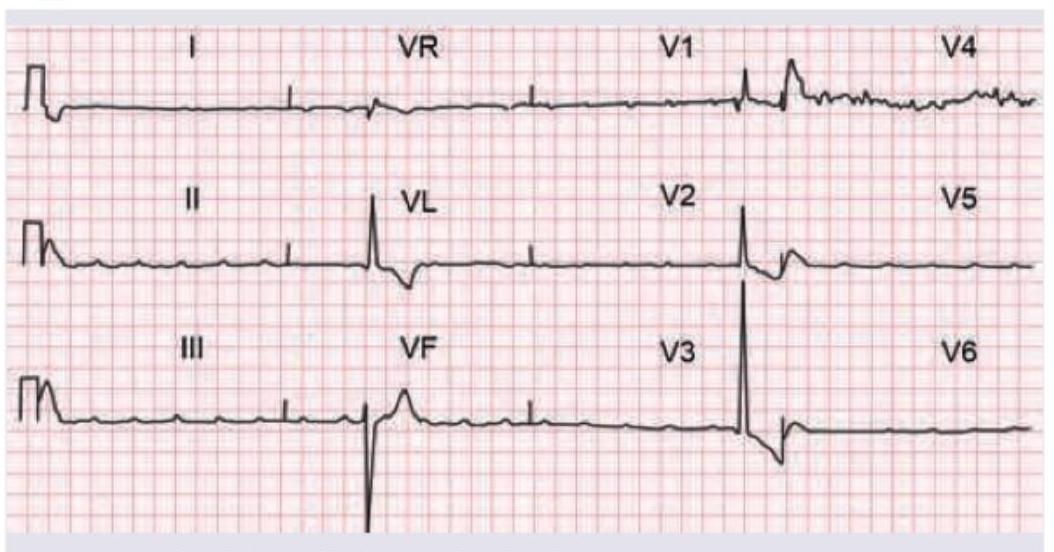
What is the axis in the ECG provided?
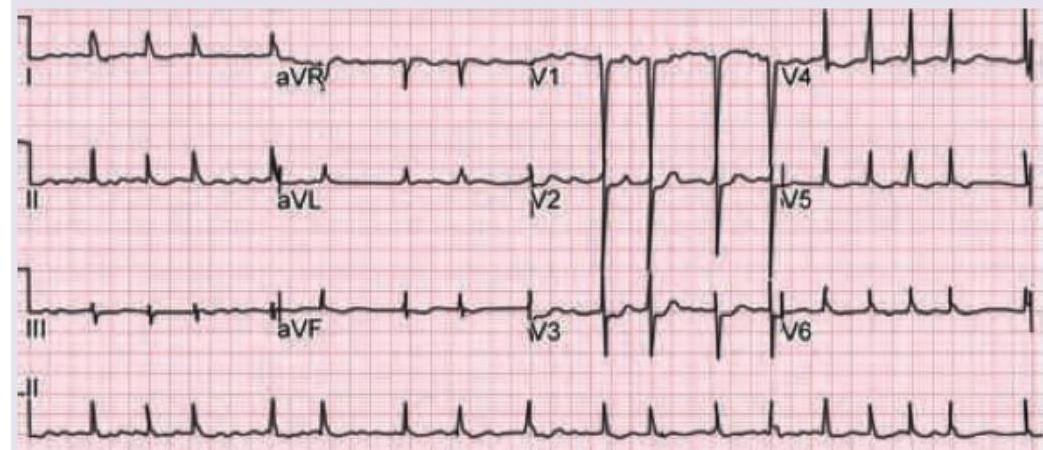
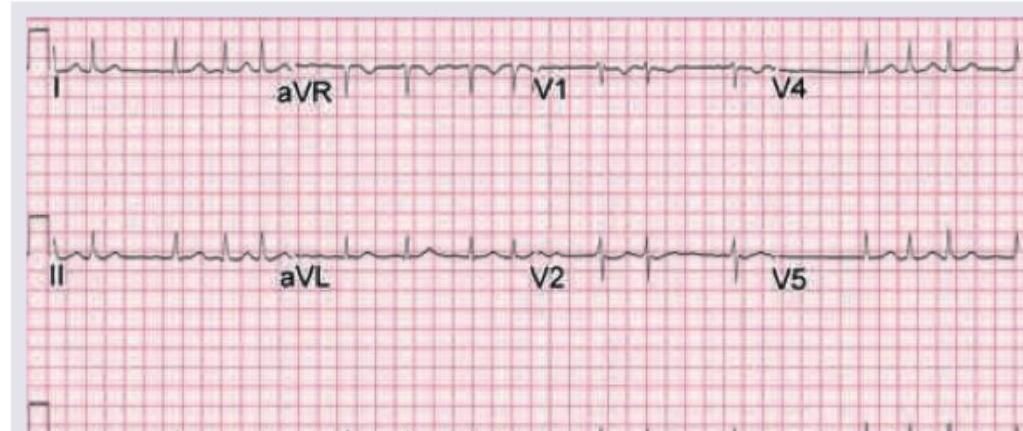
A 50-year-old woman with rheumatic heart disease is on medication for heart disease. She feels unwell for most part of the day. Which of the following medicine is responsible for the ECG changes shown below? (Recent NEET Pattern 2016-17)
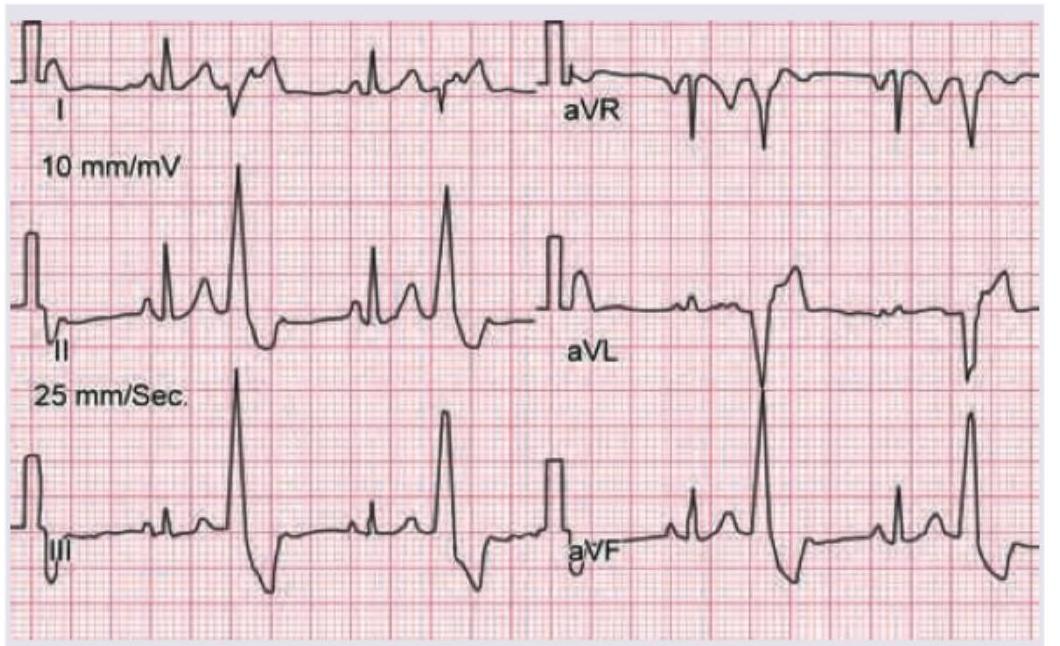
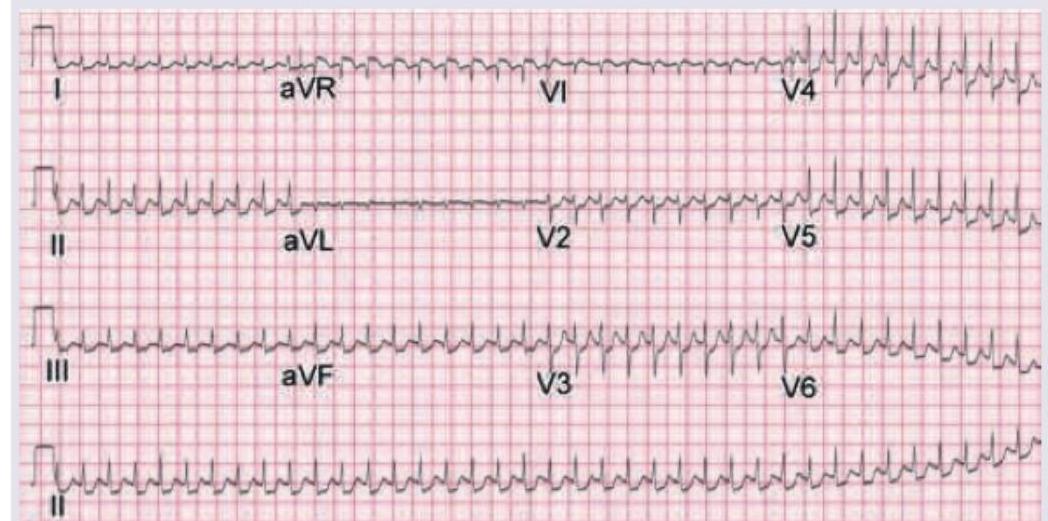
A 10-year-old child with Valvular heart disease on heart failure treatment, has the following ECG tracing. What is the diagnosis?
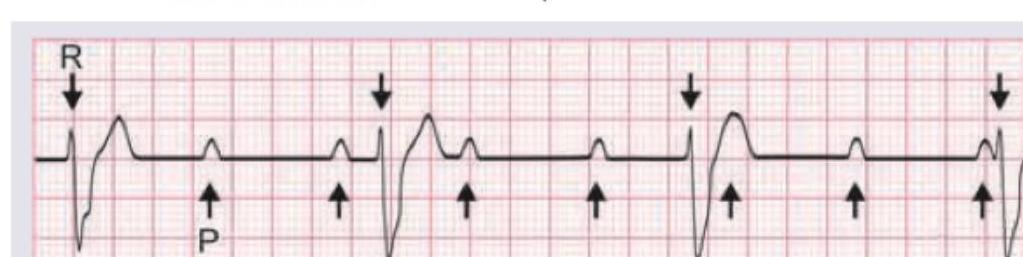
After thrombolysis for an inferior myocardial infarction, a patient develops intermittent missed beats. A rhythm strip shows progressive prolongation of the PR interval with each successive beat until a P wave is not followed by a QRS complex; the cycle then repeats. What is the most likely diagnosis?
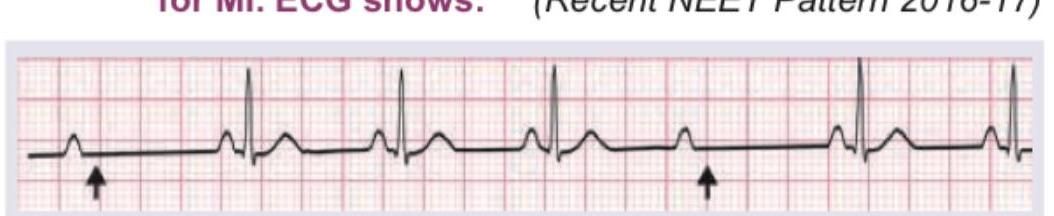
Comment on the diagnosis.
A 60-year-old patient is having recurrent syncopal attacks post myocardial infarction. The ECG shows:

Cannon A waves are seen in the JVP of a patient. ECG shows:
A 56-year-old woman presents with word-finding difficulty and hand weakness for 1 hour. ECG was done to find cause of TIA. ECG shows:
Identify the ECG finding shown below:
A 75-year-old male patient presents to the AIIMS emergency with retrosternal chest pain for 6 hours. The following ECG was done. The catheterization laboratory is immediately available and primary PCI can be achieved within the recommended timeframe. What will be the primary management of the patient?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app