
Cardiology — MCQs

On this page
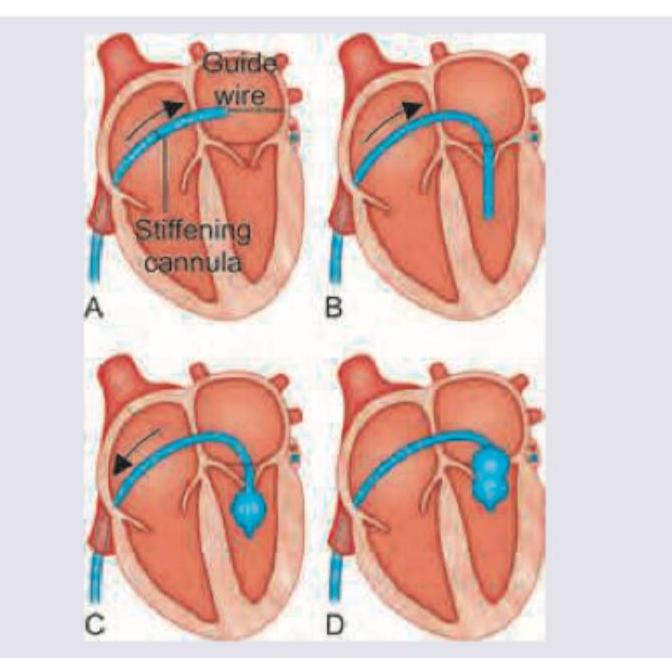
Which procedure is being performed in the image shown?
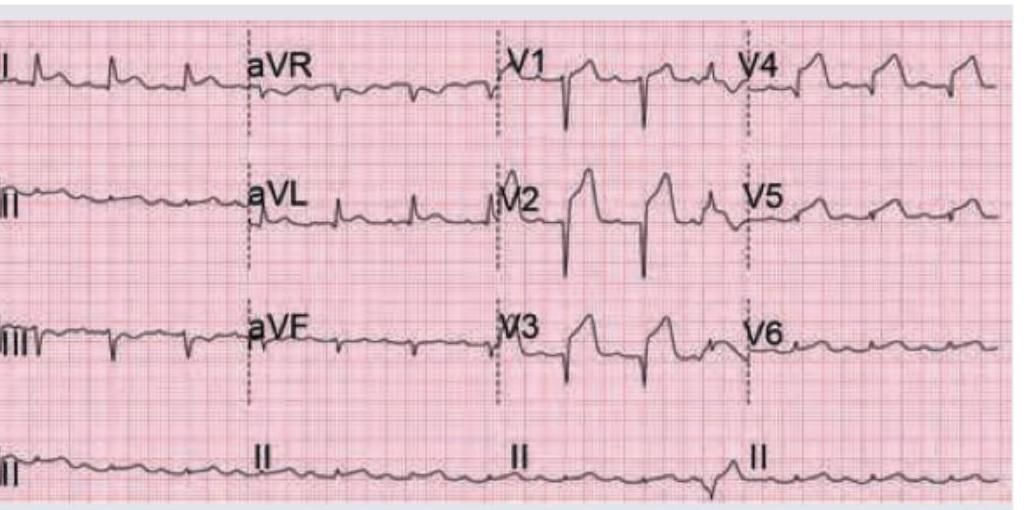
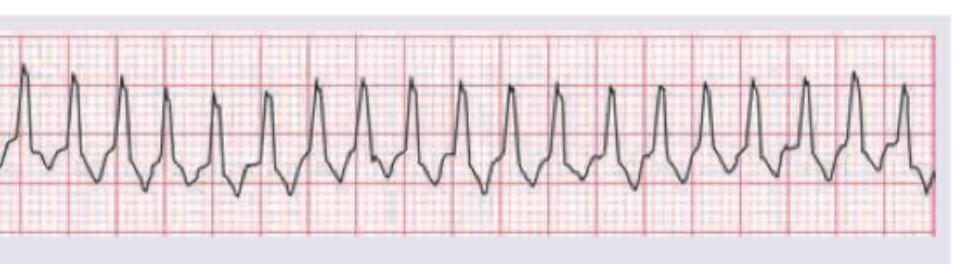
A 65-year-old diabetic presents with extensive sweating and dizziness. The ECG is shown below. What is the diagnosis?
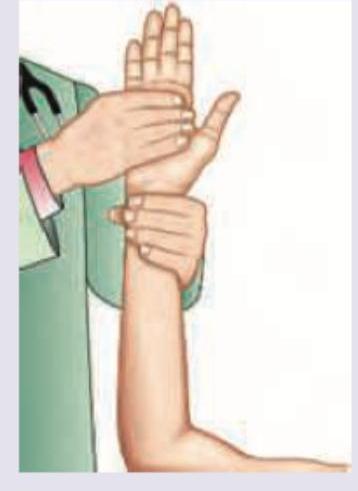
All are associated with pulse being checked in the image except:
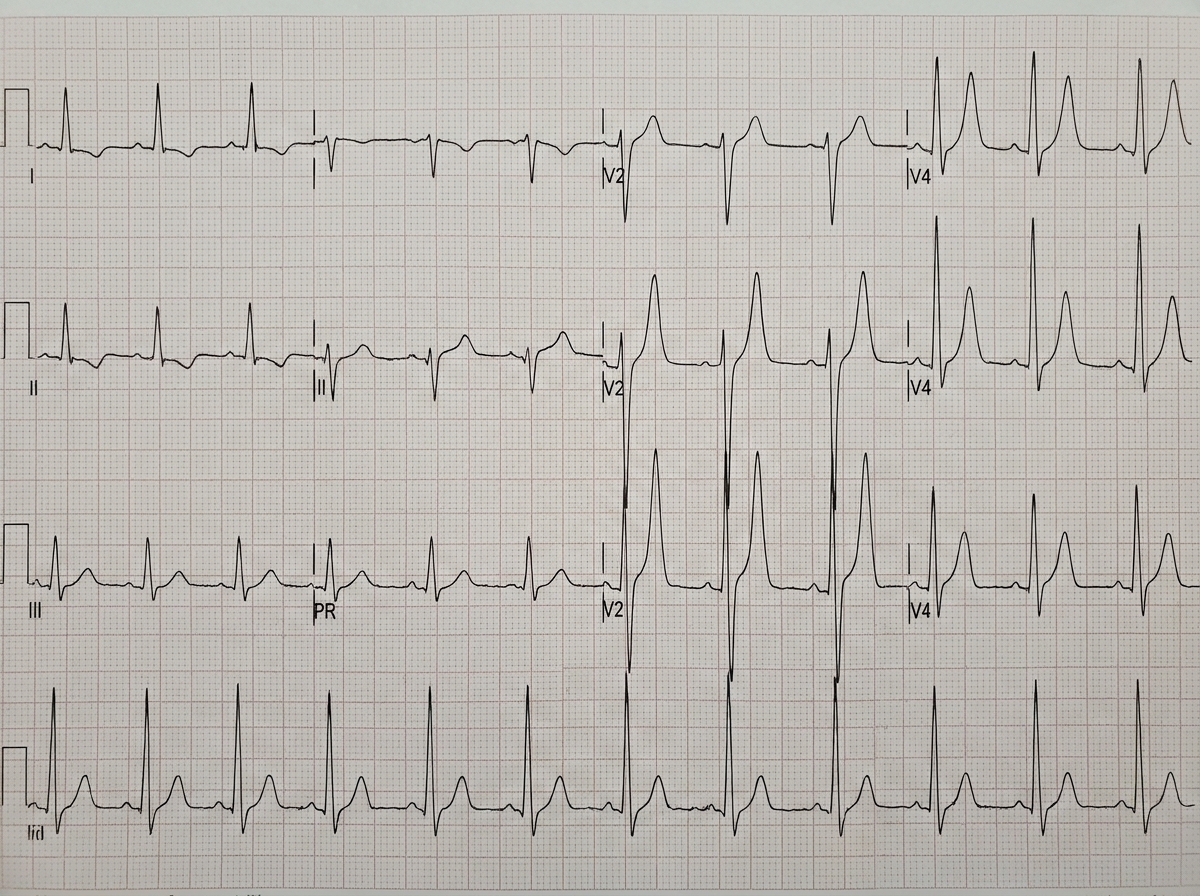
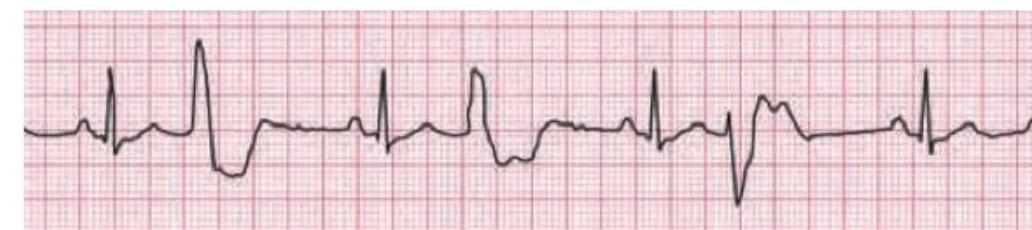
ECG shows which electrolyte abnormality?
Comment on the diagnosis of the patient?
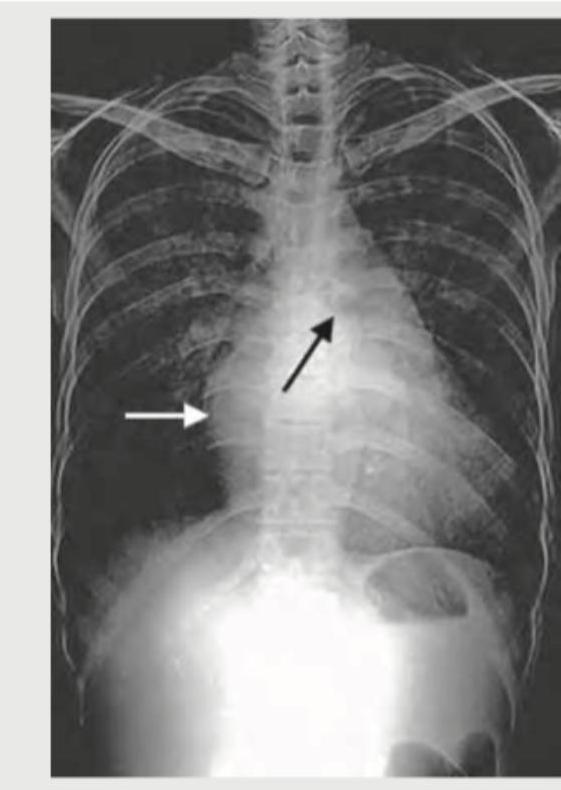
CXR was done for a 15-year-old boy with upper-extremity hypertension and weak, delayed femoral pulses. Which is incorrect about the patient?
A previously healthy patient, presents with dyspnea and low grade fever since 4 months. His lungs are clear. JVP is normal. ECG showed low voltage complexes. What is the possible diagnosis?
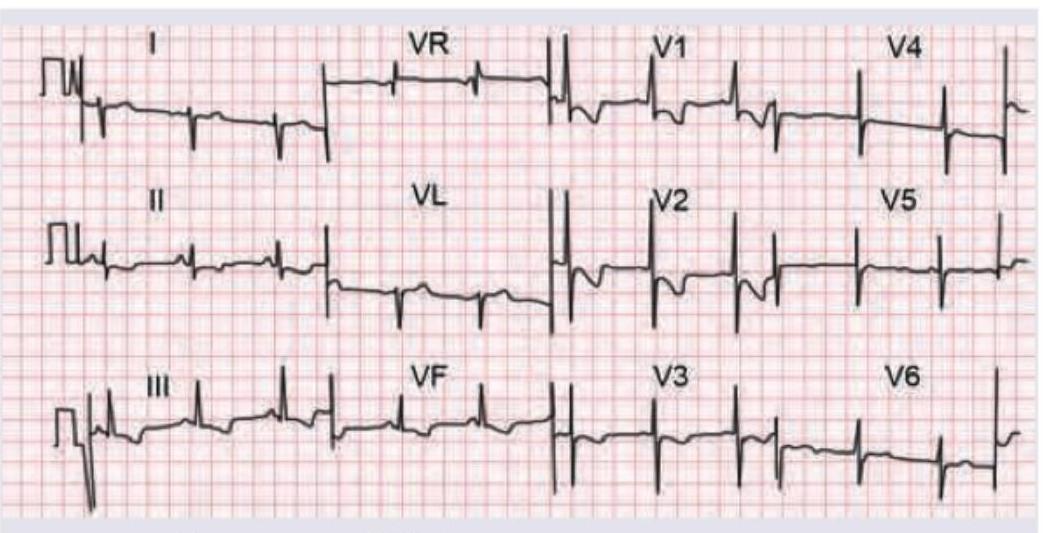
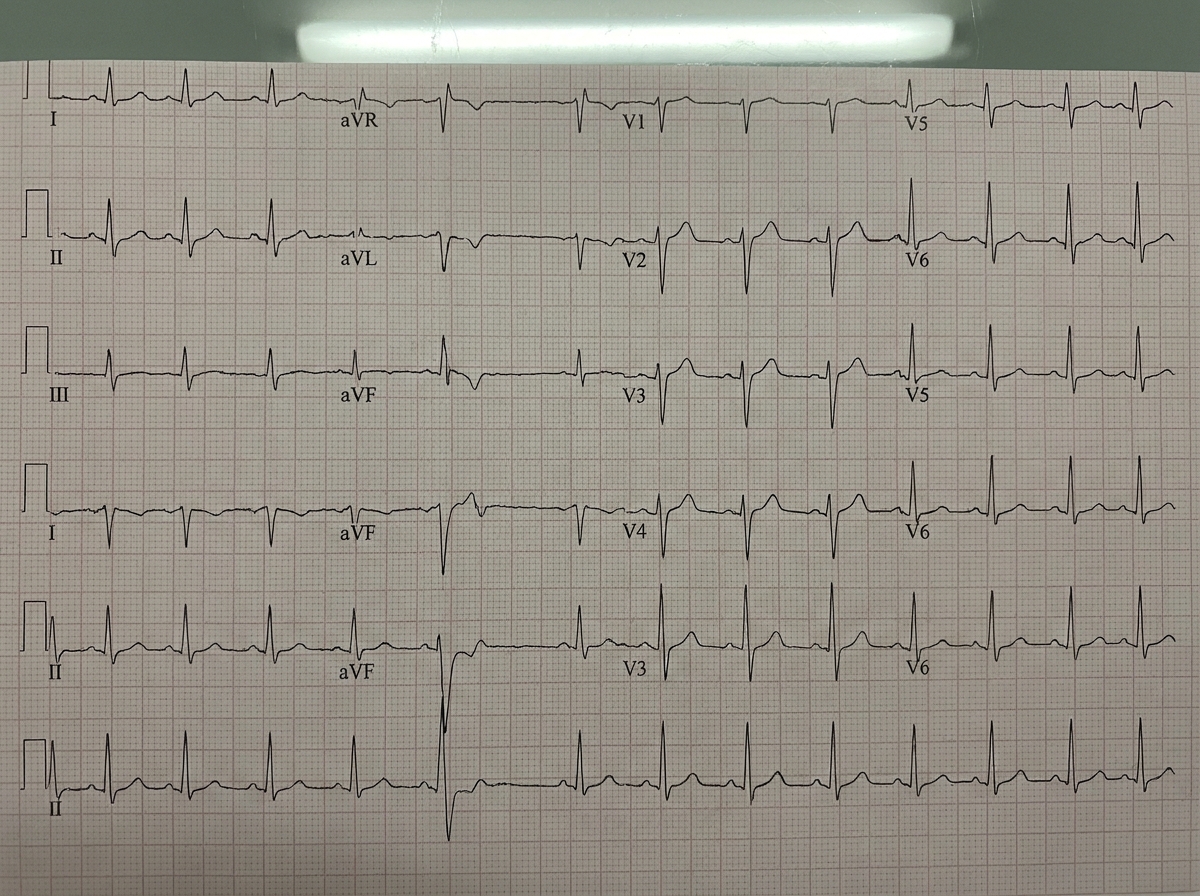
The ECG shows a heart rate of 40 bpm, left axis deviation, and QRS duration >120 msec. There are deep monophasic S waves in V1-V3, broad monophasic R waves in lateral leads I, aVL, V5-V6, and absent Q waves in lateral leads with M shaped notch in peak of R wave in V5-V6. What is the diagnosis?
A 30-year-old lady with scleroderma presents with progressive dyspnea on exertion. Which of the following is incorrect about the ECG finding?
What is the cardiac axis in the ECG provided?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app