
Cardiology — MCQs

On this page
A 58-year-old male presents to a PHC for a routine check-up. His blood pressure readings on two separate occasions are 148 / 90 mmHg and 152 / 96 mmHg. He is asymptomatic and has no known comorbidities. What is the most appropriate next step in management according to current hypertension guidelines?
A patient with recurrent episodes of PSVT (Paroxysmal Supraventricular Tachycardia) is being considered for long-term prophylactic therapy to prevent future episodes. Which of the following is the most appropriate preventive treatment?
A patient presents with palpitations and an irregularly irregular pulse. He presents within 2 hours of symptom onset, and has no history of diabetes or other comorbidities. What is the most appropriate initial management?
A 30-year-old man with 6 month past history of PND and SOB. On examination, JVP is elevated with irregularly irregular pulse and tender hepatomegaly and MDM. past medical history of ARF. Which of the following is not seen in this patient?
A patient with paroxysmal supraventricular tachycardia (PSVT) requires treatment for prophylaxis. Which drug is appropriate?
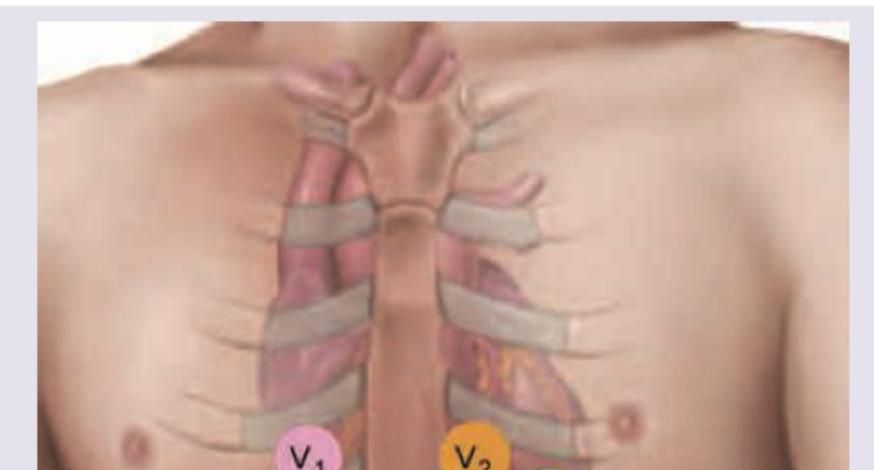
The lead of ECG marked as $X$ is called:
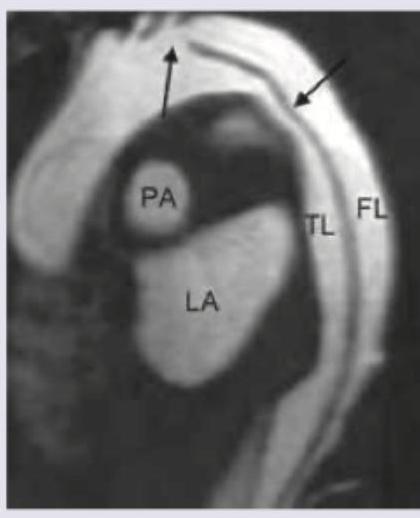
A 45-year-old patient of hypertension presents with chest pain radiating to inter-scapular area. ECG shows ST segment elevation and elevated cardiac biomarkers. Thrombolysis was initiated but patient did not improve. Cardiac MRI was performed but patient expired thereafter. All are true about the condition shown and its treatment except:
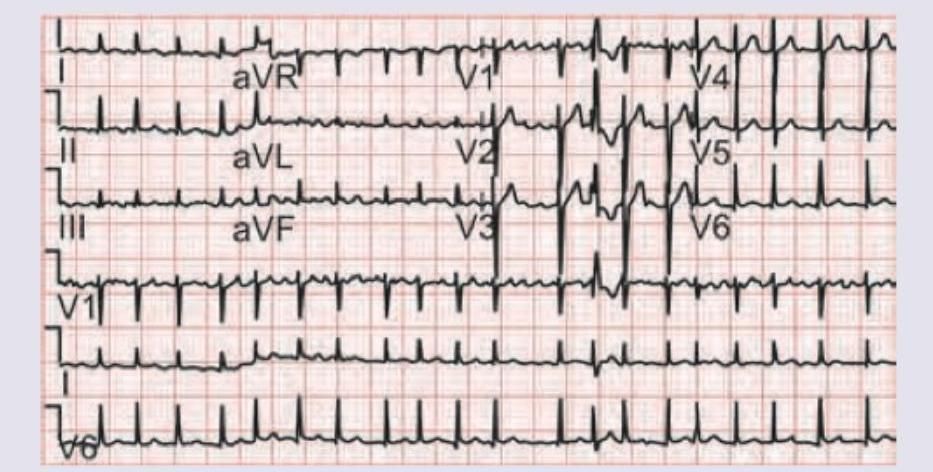
A 60-year-old hypertension patient presents with palpitations and pre-syncope. ECG was done. All drugs can be used for management of this condition except:
The image shows the dorsum of distal phalanges of the fingers of both hands approximated, leading to formation of a diamond-shaped gap — this is called Schamroth's window. Hamman crunch sign is heard in pneumomediastinum. Pemberton sign is seen in retrosternal goiter. Oliver sign is called tracheal tug and is seen in aortic aneurysm. Which of the following statements is TRUE?

What is incorrect about the condition shown in the image?

Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app