
Cardiology — MCQs

On this page
Which of the following drugs does not reduce mortality in heart failure with reduced ejection fraction (HFrEF)?
A 40-year-old woman with a history of rheumatic fever presents with shortness of breath, weight loss, fatigue, and abdominal distension. Physical examination shows rales in the lungs, hepatosplenomegaly, and 2+ pitting edema of the legs. A chest X-ray reveals only left atrial enlargement and pulmonary edema. What is the most likely cause of pulmonary edema in this patient?
All of the following are causes of a pansystolic murmur, EXCEPT?
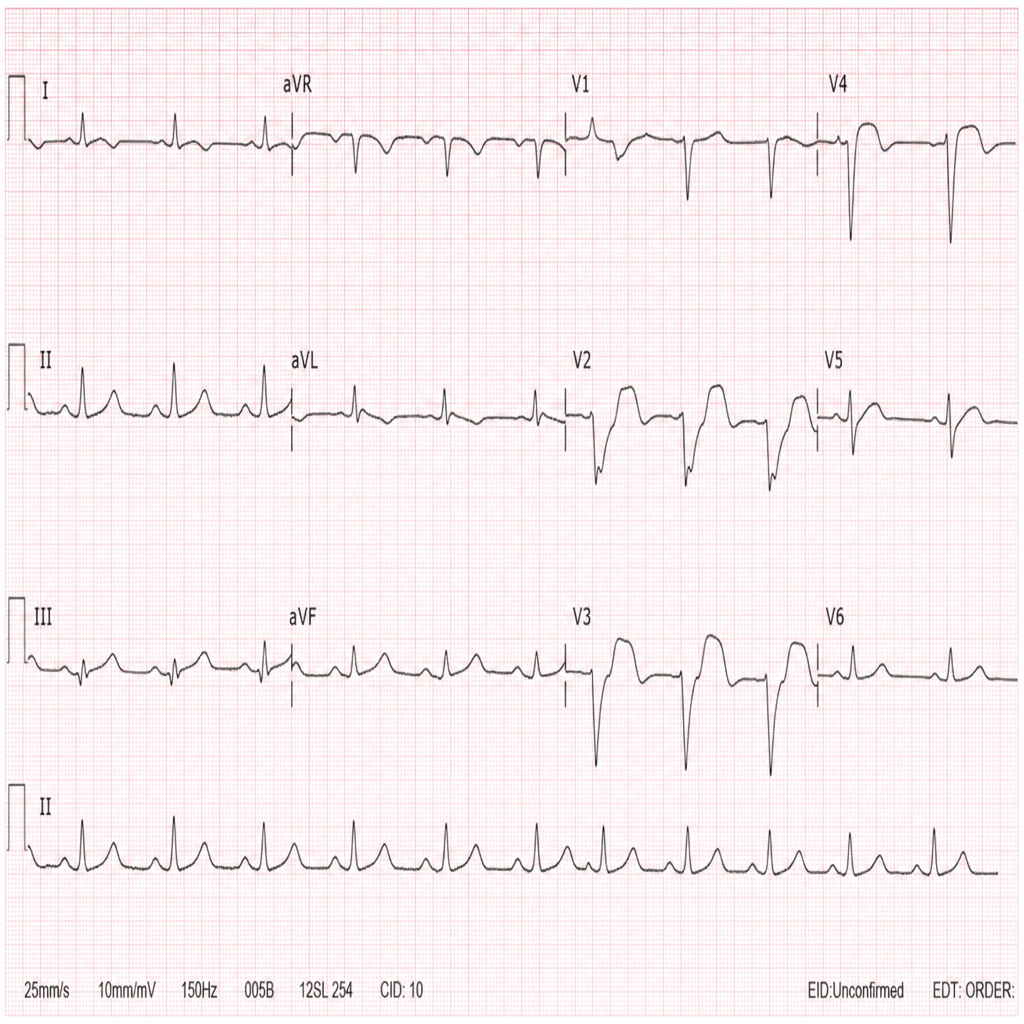
On the basis of the provided ECG, what is the most probable diagnosis?
Which of the following diseases can be associated with a short QT interval on ECG?
Blood pressure is difficult to measure in a patient with which of the following conditions?
A patient with heart failure developed ventricular arrhythmia. What is/are the appropriate treatment(s)?
Plethoric, non-collapsible IVC on echocardiography denotes?
Which of the following is NOT a cause of myocarditis?
A 50-year-old patient presents with features of poor perfusion following myocardial infarction. On examination, the heart rate is 40/min with a blood pressure of 60 mmHg systolic. Atropine was given twice over 5 minutes, but the patient's condition is not improving. What is the next best step?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app