
Cardiology — MCQs

On this page
A patient with heart failure developed recurrent sustained monomorphic ventricular tachycardia. What is/are the appropriate treatment(s)?
In a patient with mitral stenosis, disappearance of Loud S1 is associated with all except?
All of the following are features of Mobitz type I block except?
What ECG change is seen in hypocalcemia?
Amyloidosis of the heart presents with which of the following?
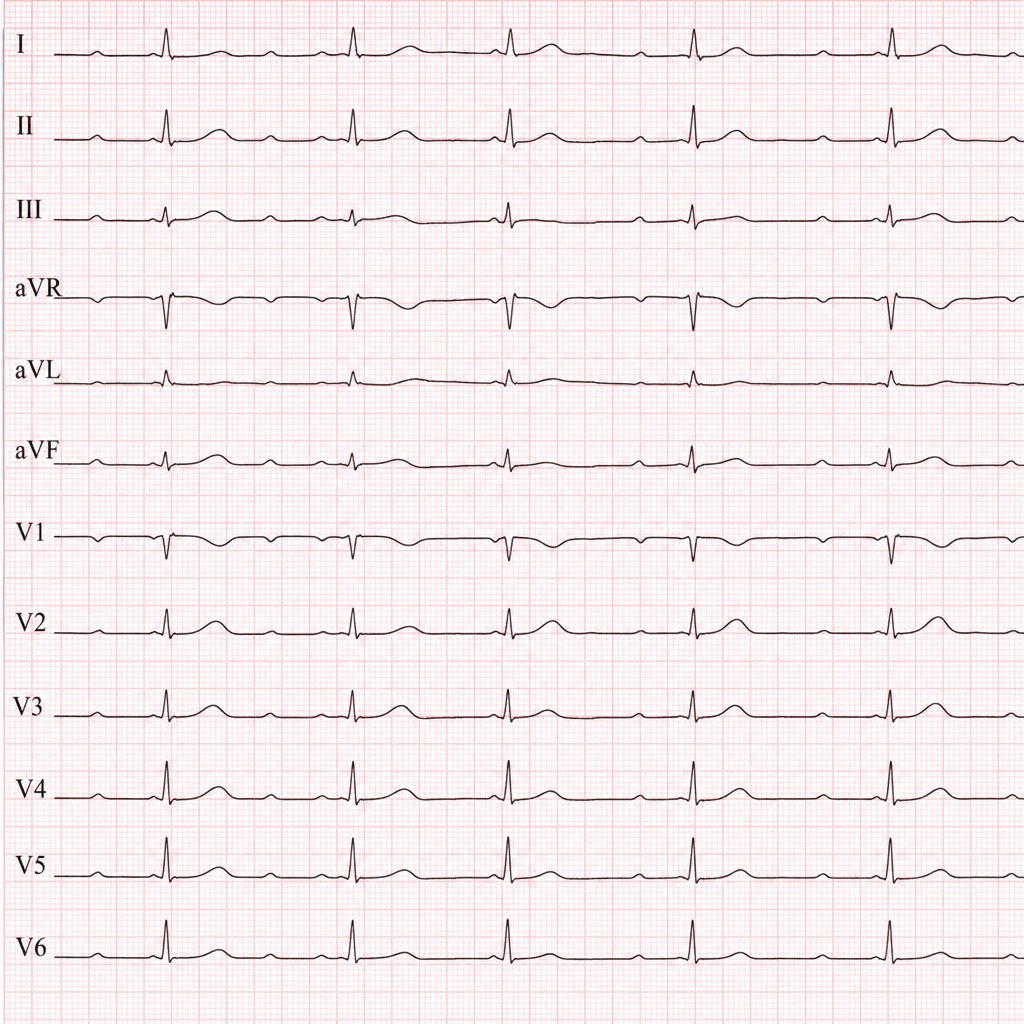
An elderly female presented to the emergency room in an unconscious state. She has a history of similar episodes in the past few months. An ECG was performed, and the resulting graph is provided. Which of the following is the most probable cause?
A 78-year-old woman presents with an acute anterior wall myocardial infarction, accompanied by hypotension and pulmonary congestion. Her blood pressure is 90/70 mm Hg, pulse is 110/min, JVP is at 8 cm, and heart sounds are normal. The lungs exhibit bibasilar crackles, and her extremities are cool and diaphoretic. What would central hemodynamic monitoring most likely reveal in this patient?
A 63-year-old woman with a history of aortic stenosis and left ventricular hypertrophy experienced cardiac arrest and died. Which of the following predisposes to sudden cardiac death?
Brugada syndrome is characterized by what ECG finding?
A 70-year-old man with hypertension presents with severe chest pain and diaphoresis. On examination, he has bounding pulses with wide pulse pressure. A diastolic murmur is heard along the right sternal border. Which of the following is the possible etiology?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app