
Cardiology — MCQs

On this page
A 69-year-old male, a heavy smoker (60 cigarettes/day for 40 years), presented with a 12-hour episode of slurred speech that resolved. He had a single episode of haemoptysis 4 weeks prior and has known lung cancer with brain metastases. An ECG revealed new atrial fibrillation, and all blood tests, including cardiac biomarkers, were normal. A chest CT was performed. Based on the clinical presentation and CT findings, which of the following is the most probable diagnosis?
A 67-year-old man with an 18-year history of type 2 diabetes mellitus presents for a routine physical examination. His temperature is 36.9 C (98.5 F), his blood pressure is 158/98 mm Hg and his pulse is 82/minute and regular. On examination, the physician notes a non tender, pulsatile, mass in the mid-abdomen. A plain abdominal x-ray film with the patient in the lateral position reveals spotty calcification of a markedly dilated abdominal aortic wall. Following surgery, the patient is placed on a low-fat diet to reduce the risk of continued progression of his atherosclerotic disease. A bile acid sequestrant is added to interrupt enterohepatic circulation of bile acids. Which of the following agents was MOST likely prescribed?
In Mitral Valve Prolapse (MVP), which of the following conditions would cause the ejection click to be more accentuated and the murmur to move closer to the first heart sound?
A "third heart sound" is heard in all of the following conditions EXCEPT?
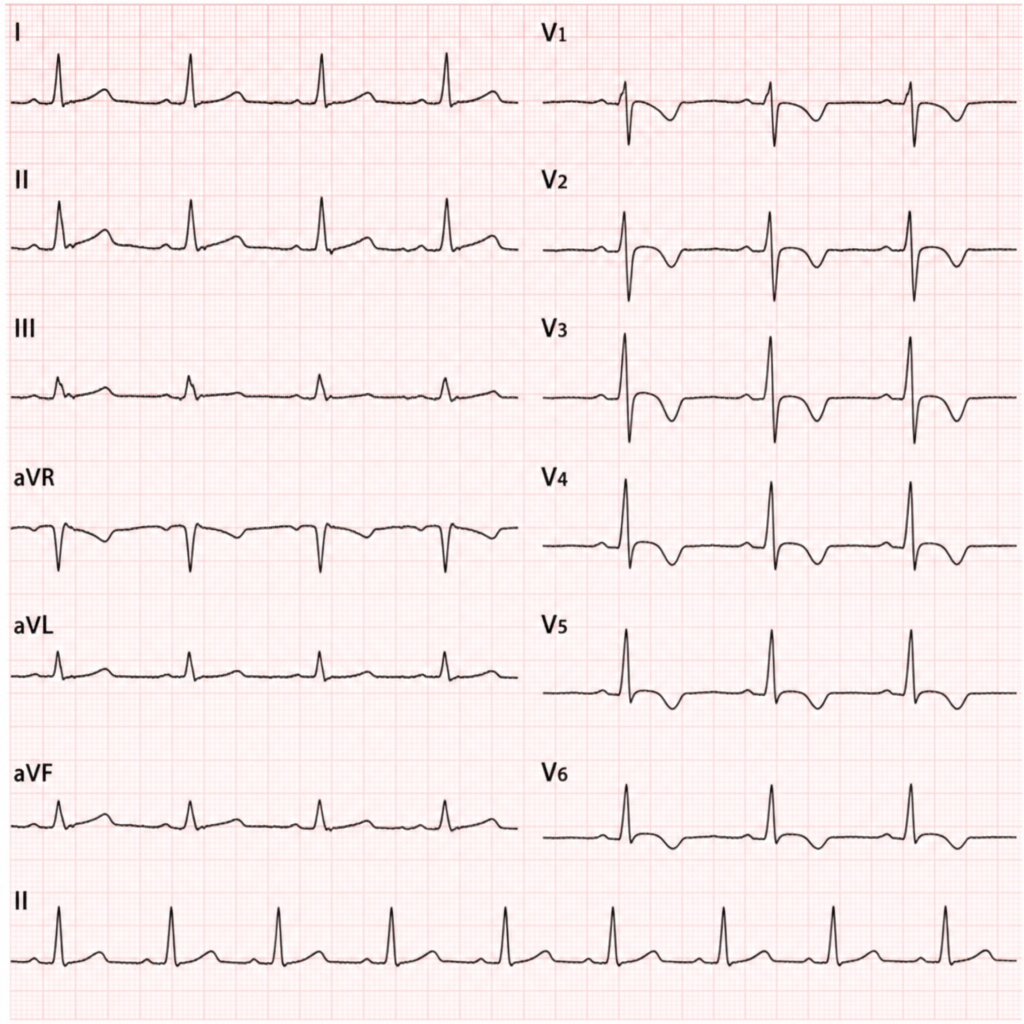
Which of the following findings is shown in the chest leads?
Which of the following is true about the third heart sound?
Which features favor constrictive pericarditis over restrictive cardiomyopathy?
What is the most common cause of Left Ventricular Hypertrophy?
A 60-year-old woman presents with a murmur suggestive of mitral stenosis and an echocardiography confirmed a mass attached to the fossa ovalis of the left atrial septum. What is the most likely diagnosis?
Wide pulse pressure is seen in which of the following conditions?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app