
Cardiology — MCQs

On this page
What is the preferred analgesic for pain associated with ST-elevation myocardial infarction (STEMI)?
All of the following are usual features of left atrial myxoma, except?
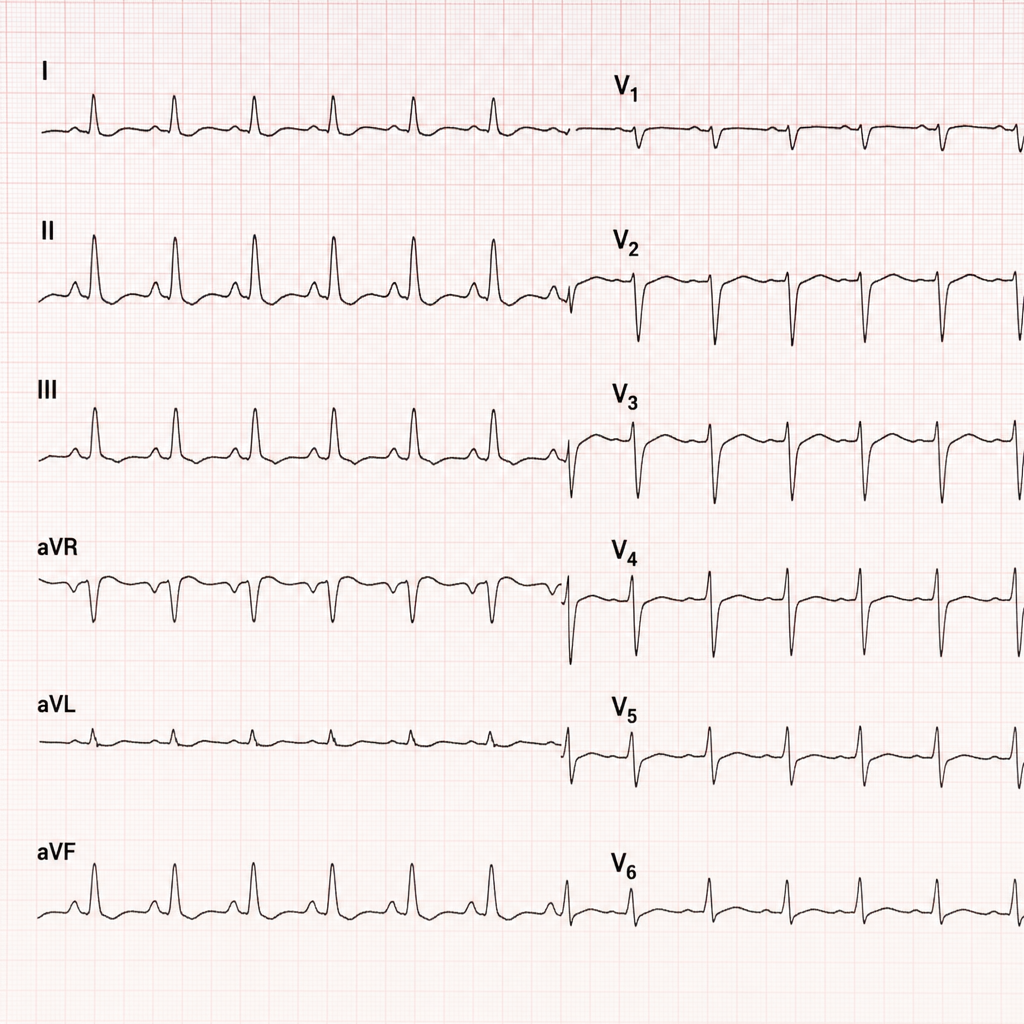
The following ECG represents?
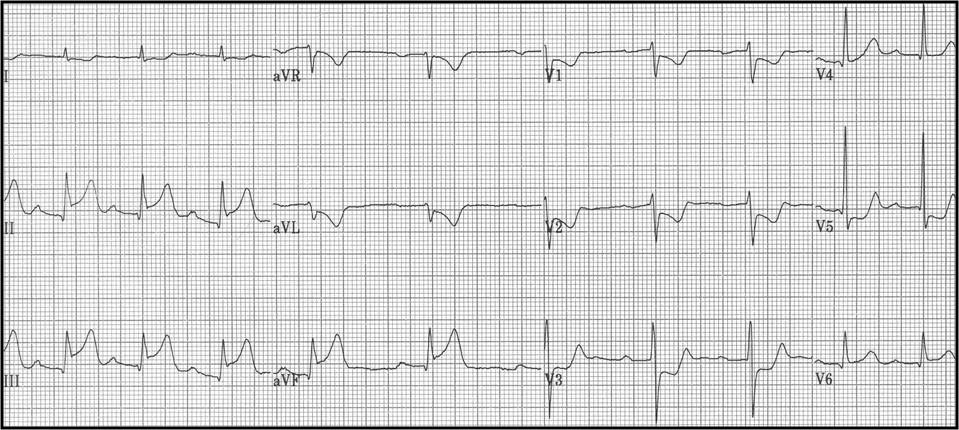
Which coronary artery is the most likely culprit for the inferior STEMI seen on the ECG shown below?
Pulsus paradoxus is seen in which of the following conditions?
Recurrent ischemic events following thrombosis have been pathophysiologically linked to which of the following?
Paradoxical splitting of the second heart sound is heard in which of the following conditions?
A 50-year-old female presents to the OPD with shortness of breath. On examination, she is hypotensive, has soft heart sounds, and elevated JVP. Her ECG shows a reduction in the amplitude of QRS complexes. Which of the following is the investigation of choice for diagnosing her condition?
All of the following are clinical features of myxoma, EXCEPT:
An electrocardiogram (ECG) in a patient with a systolic ejection murmur that shows an incomplete bundle branch block in the precordial lead is most consistent with which of the following conditions?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app