
Cardiology — MCQs

On this page
Reperfusion is believed to restore contractile function of which of the following?
A 71-year-old man presents with blurry vision and blood-tinged urine. He has a history of hypertension treated with a beta-blocker, an ACE inhibitor, and a calcium channel blocker. His symptoms began 3 days ago when he stopped his medications. His blood pressure is 200/110 mmHg, funduscopic examination reveals flame hemorrhages and papilledema, and urinalysis shows red blood cells with dysmorphic red blood cell casts. He has an abdominal bruit. What is the most appropriate next step in management?
Which of the following is a criterion for cardiac shock?
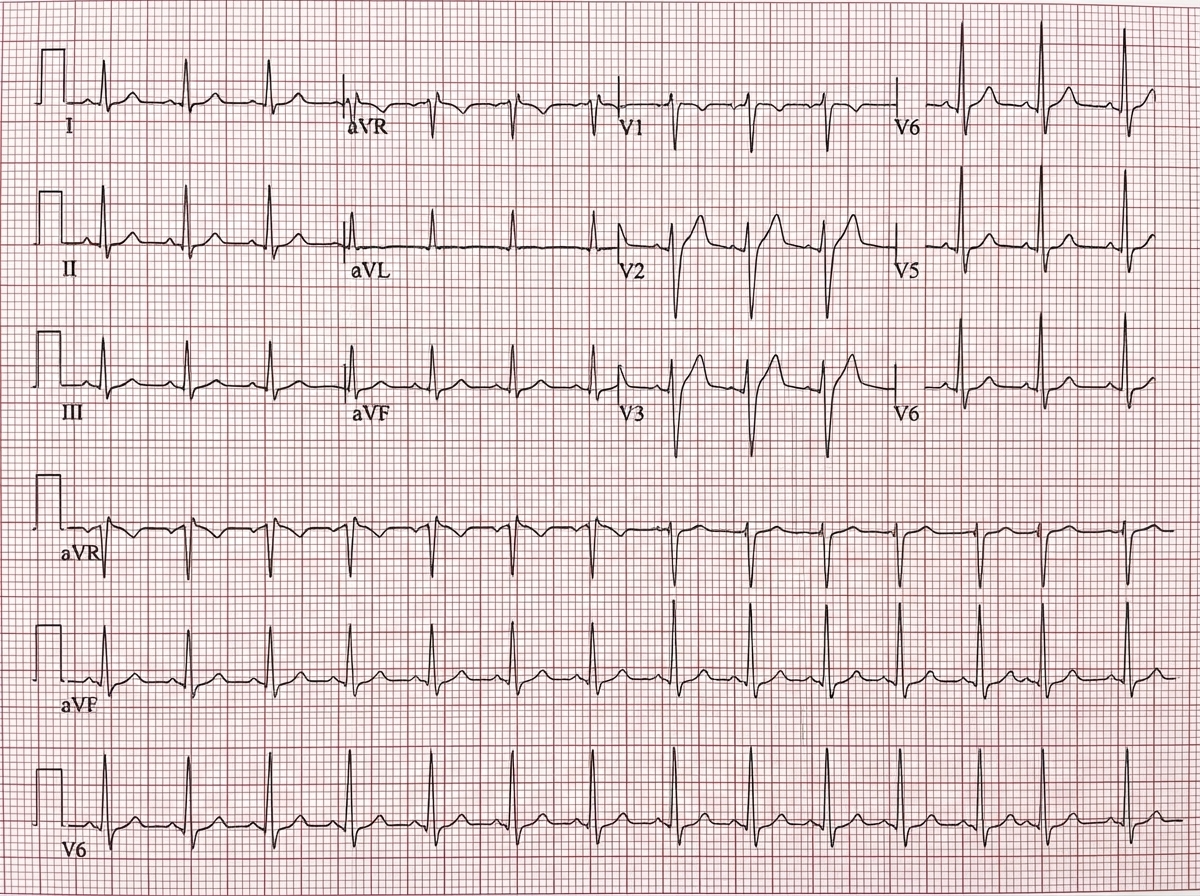
A 26-year-old man attends an occupational health assessment. A 12-lead ECG is recorded. He is feeling well and has no symptoms or significant past medical history. Based on the ECG findings, what is the most likely diagnosis?
Which of the following investigations can detect the volume of infarcted area in acute myocardial infarction?
Brugada syndrome is associated with which of the following ECG findings?
All of the following can occur in rheumatic fever except?
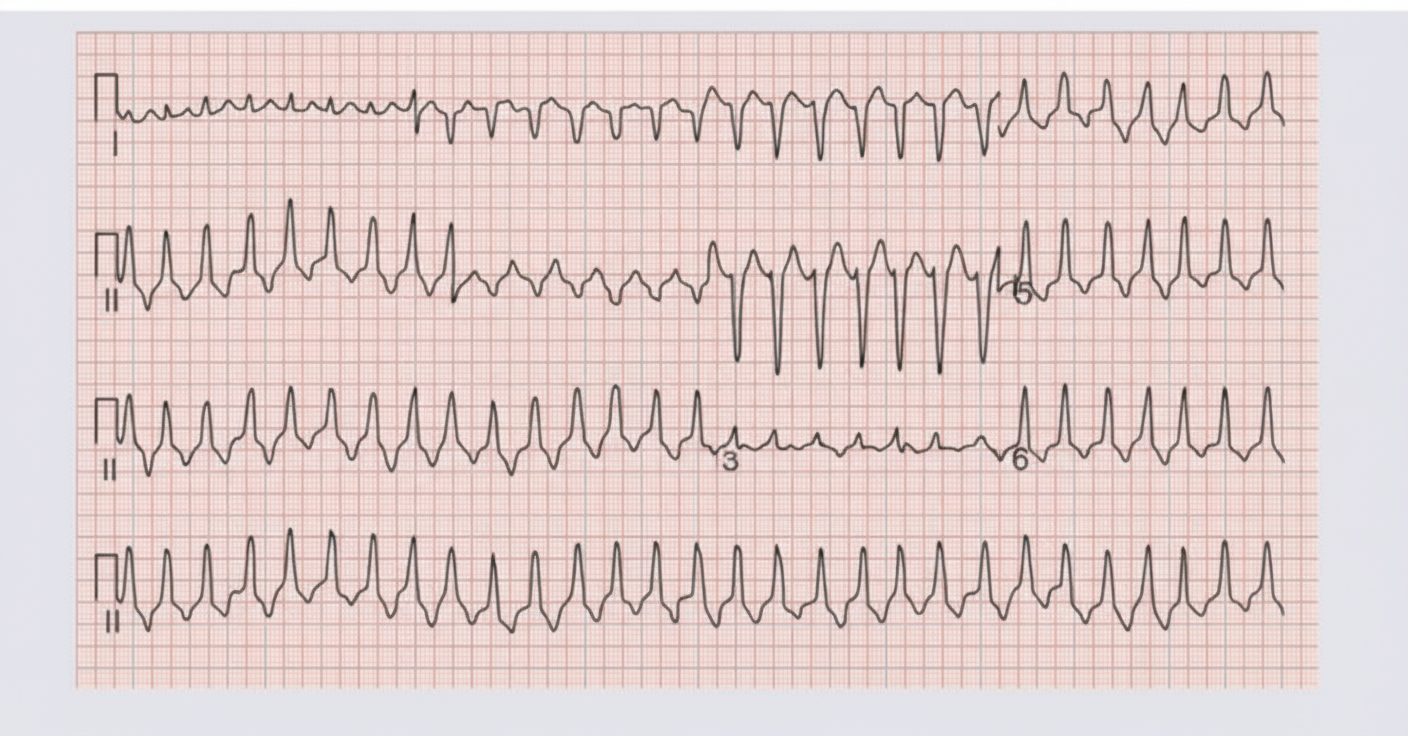
A 70-year-old male with a history of hypertension and diabetes mellitus presents with the following rhythm, accompanied by a blood pressure of 90/40 mm Hg and a feeble pulse. What is the next step in management?
A patient with myocardial infarction presents with nausea, vomiting, epigastric pain, and bradycardia. ECG shows a first-degree heart block. What is the most commonly involved coronary artery in this scenario?
Which of the following is NOT true about Hypertrophic Obstructive Cardiomyopathy?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app