
Cardiology — MCQs

On this page
A 55-year-old male with a history of type 2 diabetes mellitus, managed with oral hypoglycemic agents, presents with a blood pressure reading of 164/102 mm Hg. What is the most suitable antihypertensive drug for this patient?
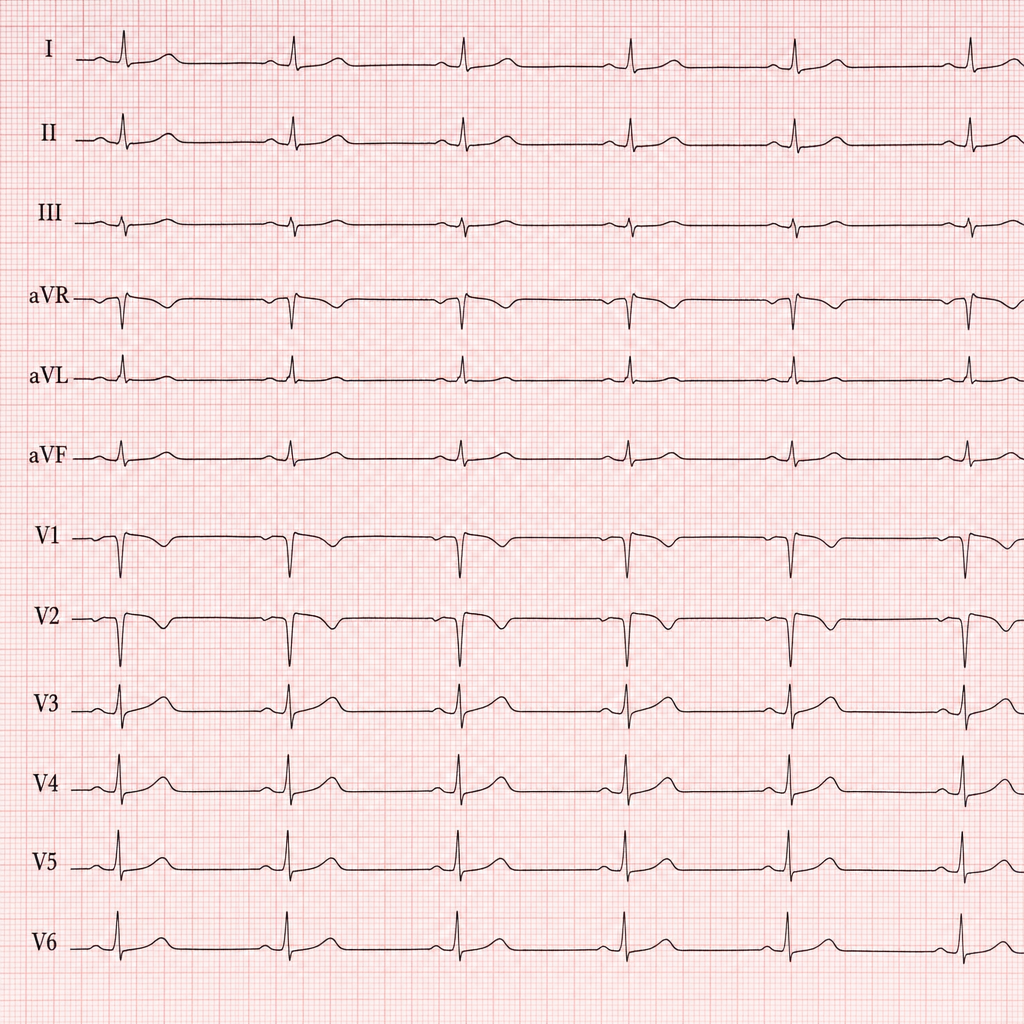
A 65-year-old man is about to undergo an elective hip replacement. A pre-operative ECG is taken. Based upon the ECG, which of the following jugular venous pressure (JVP) abnormalities is most likely to be present?
A 48-year-old male patient with an anterior myocardial infarction underwent primary angioplasty with a bare metal stent. What duration of antiplatelet therapy will you advise for discharge?
A patient in regular rhythm presents with absent P waves on ECG. Leads II, III and aVF reveal a saw-tooth pattern. Which of the following is the most likely diagnosis?
Infective endocarditis is common in which of the following conditions?
What is the commonest congenital lesion complicated by infective endocarditis?
A 75-year-old man presents with a syncopal episode. He had no incontinence or post-event confusion. Examination reveals a blood pressure of 140/80 mm Hg, pulse of 72/min with no postural changes. His second heart sound is diminished, and there is a systolic ejection murmur that radiates to the carotids. The Valsalva maneuver decreases the murmur's length and intensity. What is the most likely diagnosis for this patient's systolic murmur?
A 36-year-old male presents with a 2-day history of continuous chest pain that does not change with activity. Vital signs reveal normal blood pressure, mild tachycardia and tachypnea, and an oxygen saturation of 90% on room air. The cardiopulmonary examination is normal. An ECG shows a rate of 106 beats/min, left axis deviation, left ventricular hypertrophy, PR depression, and T wave inversions in V2 to V5. Troponin and CPK-MB are minimally elevated. What is the most likely diagnosis?
A 64-year-old male presents with dyspnea and edema. He had previous coronary bypass surgery 5 years ago, which was uncomplicated. Since then he has had no further chest pain. On examination, his JVP is at 8 cm, with prominent Kussmaul's sign. The heart sounds are easily heard but there is an early diastolic filling sound (pericardial knock). For this patient, select the most likely diagnosis.
All of the following are electrocardiographic features of hyperkalemia, except?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app