
Cardiology — MCQs

On this page
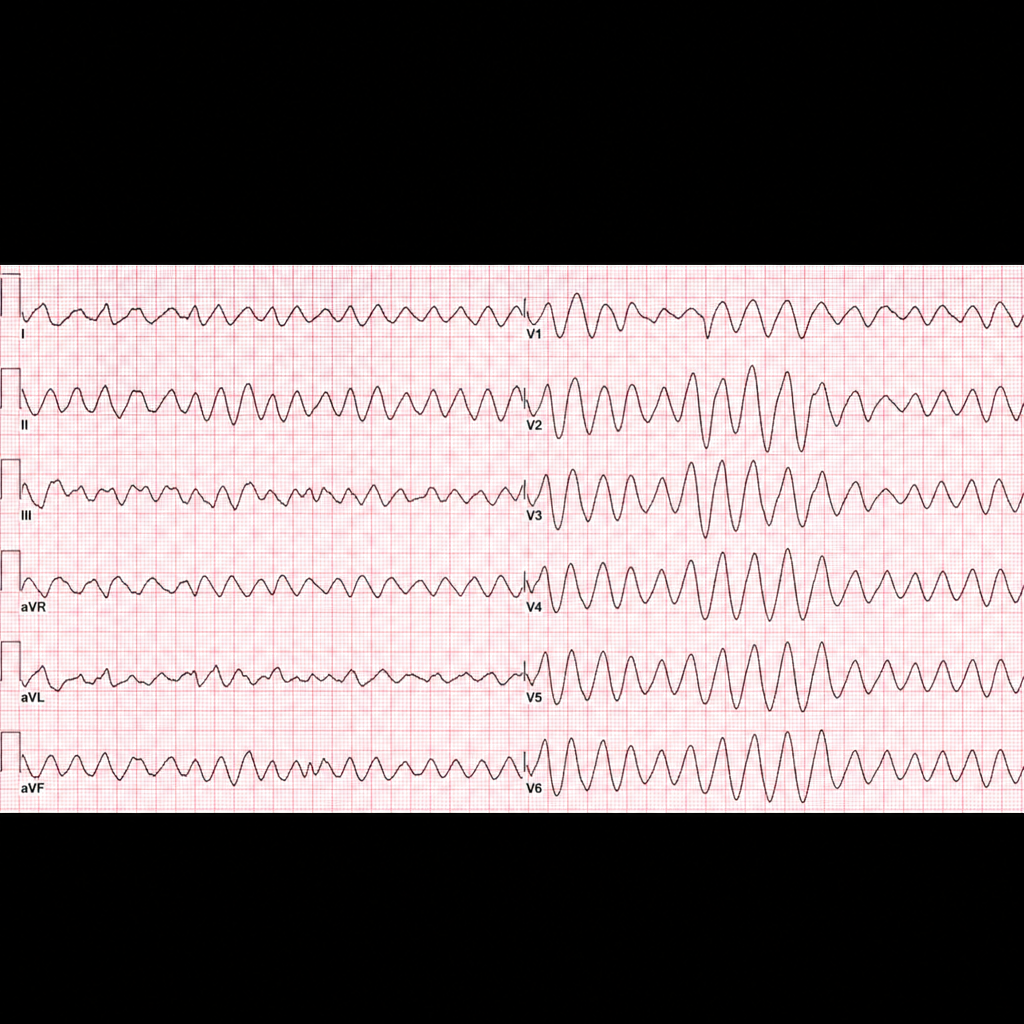
A pulseless patient in cardiac arrest has the ECG findings shown. All of the following are indicated in the management, except?
Which of the following is NOT true regarding lifestyle modifications for managing essential hypertension as recommended by the American Heart Association (AHA)?
A patient with diabetes mellitus of 4 years duration presents with dizziness and a heart rate of 52 beats per minute. What is the probable cause?
What is the investigation of choice (IOC) for cardiac tamponade?
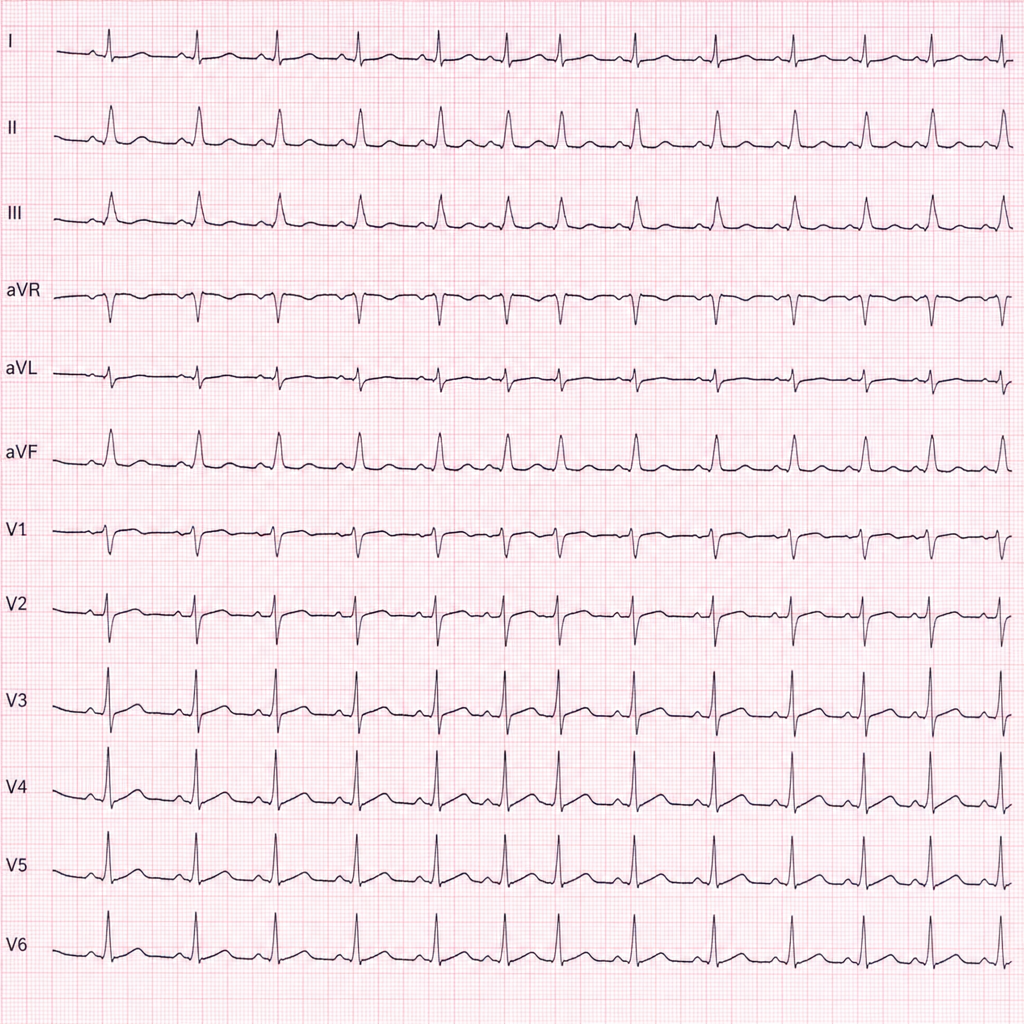
Which of the following conditions will predispose to the cardiac rhythm shown?
Which of the following is not a feature of right heart failure?
What is the initial management of newly diagnosed hypertension?
Which of the following is false regarding the Austin-Flint murmur?
What is the treatment of choice in ventricular fibrillation?
Which of the following features on X-ray chest can differentiate an Atrial Septal Defect (ASD) from a Ventricular Septal Defect (VSD)?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app