
Cardiology — MCQs

On this page
Which of the following produces a continuous murmur except?
Pulsus paradoxus is seen in all of the following EXCEPT:
A 55-year-old woman presents with complaints of chest pain. She states that the chest pain predictably occurs when she climbs four flights of stairs to reach her apartment or when she has been jogging for more than 10 minutes. She is particularly concerned because her mother died of a myocardial infarction at 50 years of age. Which of the following best describes this patient's state?
What is the most likely cardiac lesion in a young adult who complains of headache, dizziness, and intermittent claudication with exercise?
A 65-year-old man with a history of syncopal attacks on exertion and angina is undergoing heart valve surgery. Which kind of pulse is expected to be present before surgery?
A 63-year-old woman develops exertional angina and has had two episodes of syncope. Examination shows a systolic ejection murmur with radiation to the carotids and a soft S2. Which of the following is the most likely diagnosis?
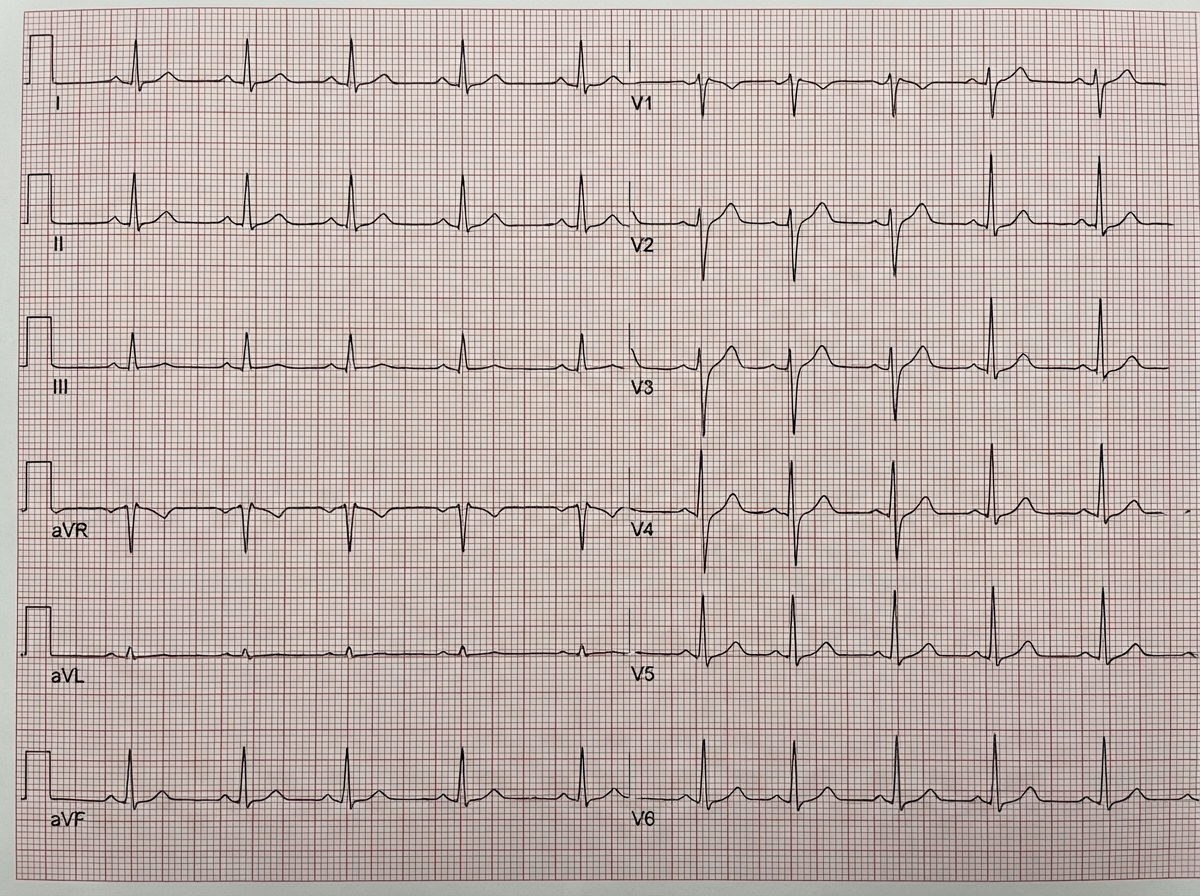
Which of the following is NOT included in the differential diagnosis of this ECG finding?
In which condition is the intensity of a systolic murmur increased?
A 35-year-old athlete has height 184 cm, arm span 194 cm, pulse rate 64/min, and BP 148/64 mm Hg. Chest auscultation reveals a long diastolic murmur over the right second intercostal space on routine examination. What is the probable diagnosis?
Which of the following is the most common identifiable cause for restrictive cardiomyopathy?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app