
Cardiology — MCQs

On this page
What is the most appropriate intervention for acute myocardial infarction?
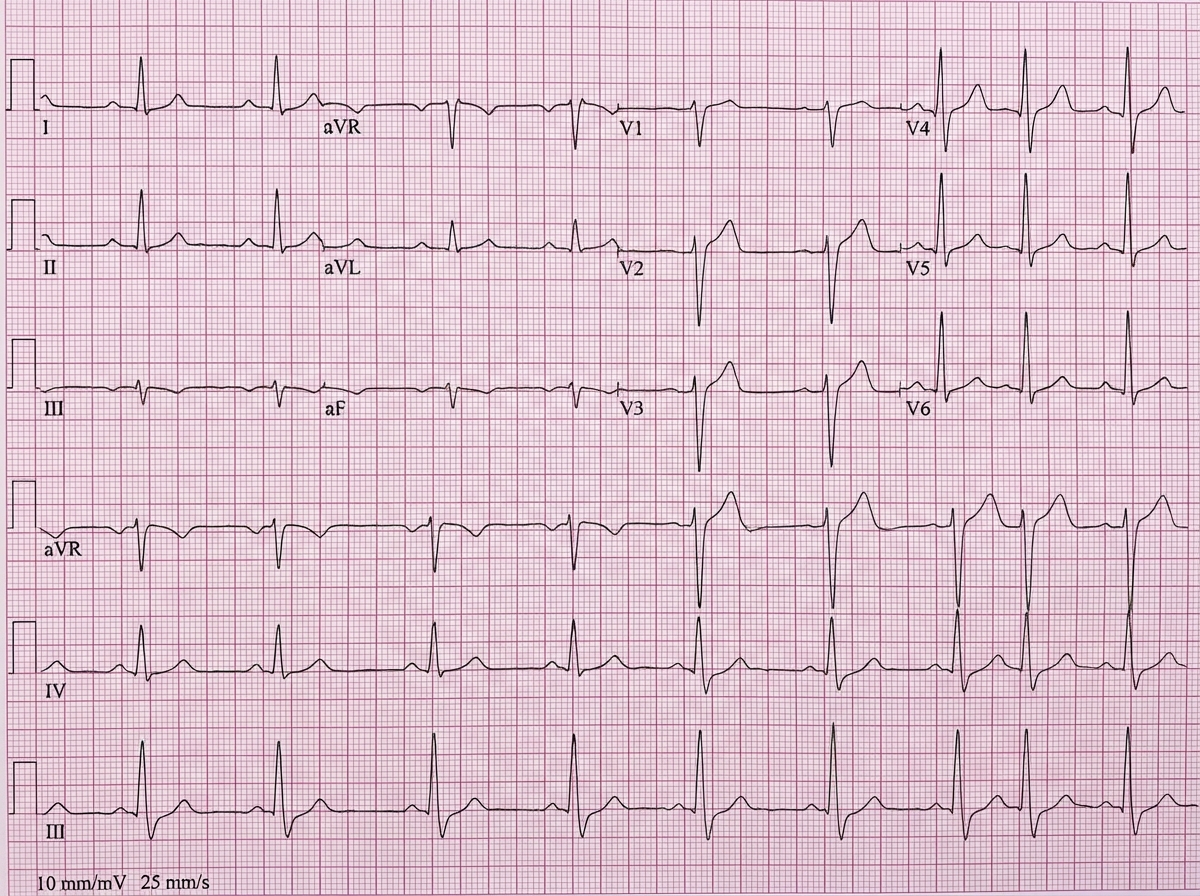
What is the abnormality shown in the ECG?
Pulsus bisferiens is seen in all except?
Which of the following arrhythmias is most frequent in Holiday Heart Syndrome?
Protein-losing enteropathy is seen in which of the following conditions?
A 73-year-old man has angina pectoris on exertion, but an angiogram reveals noncritical stenosis of the coronary arteries. This clinical presentation is most frequently associated with which of the following valvular heart diseases?
A patient with acute inferior wall myocardial infarction has developed shock. Which of the following is the most likely cause of shock?
Which of the following is not a major Framingham criterion for heart failure?
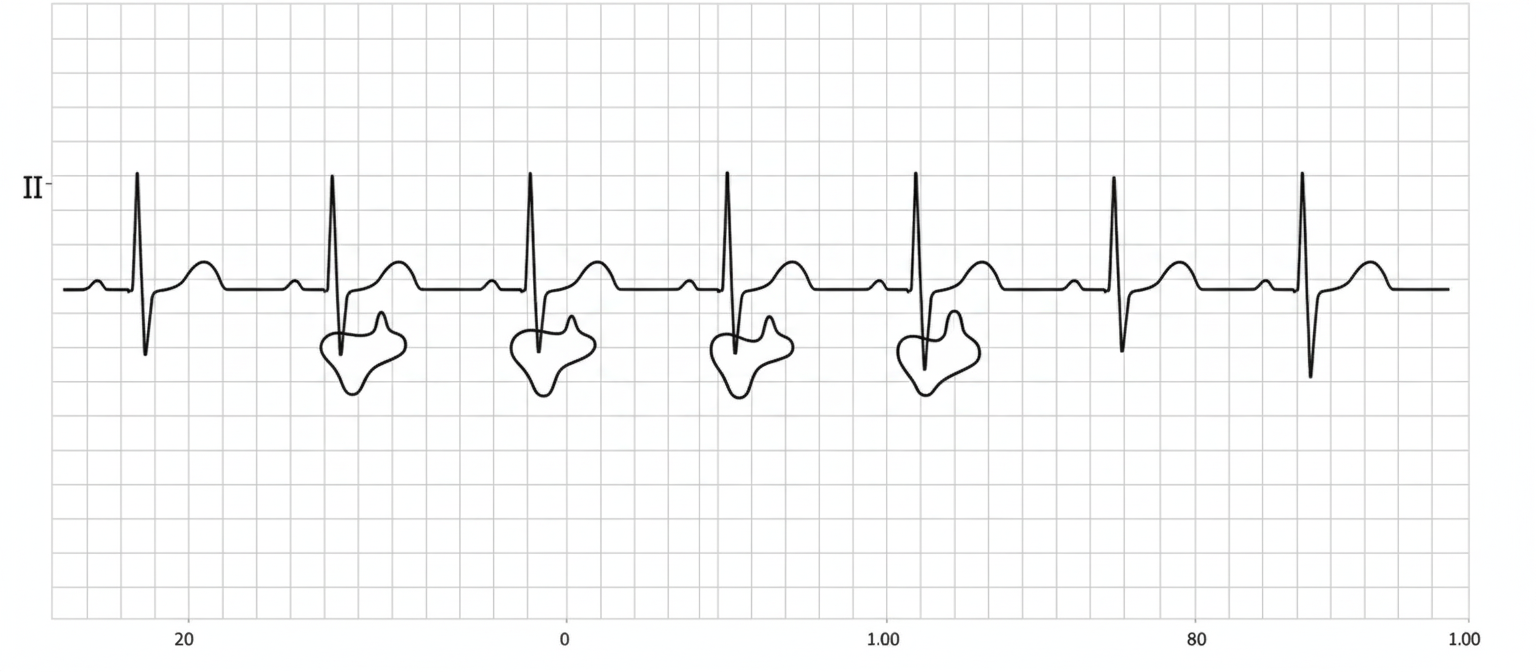
A 70-year-old man with a past medical history of ischemic heart disease and hypertension presents to his GP with recurrent episodes of syncope over the past 2 weeks. Based upon this ECG, which of the following JVP findings is most likely to be present?
Atrial fibrillation may occur in all of the following conditions, except?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app