
Cardiology — MCQs

On this page
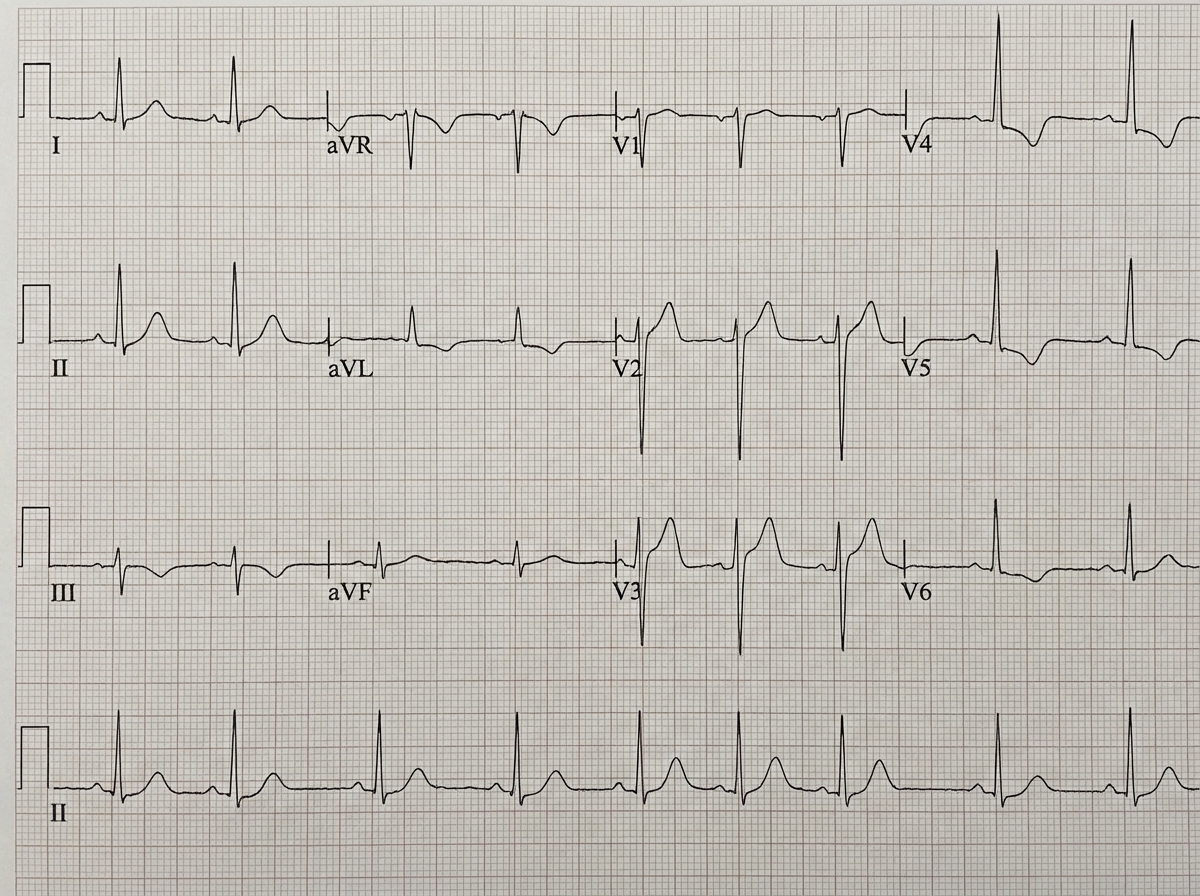
In which electrolyte abnormality, the following ECG finding is seen?
A 55-year-old man presents with gradually increasing shortness of breath and leg swelling over the past month. He has orthopnea and paroxysmal nocturnal dyspnea. His medical history includes hypercholesterolemia treated with simvastatin and hypertension treated with hydrochlorothiazide. Current blood pressure is 140/90 mm Hg. Physical examination reveals mild jugular venous distension, bibasilar crackles, an S3 gallop, and minimal pedal edema. Echocardiography shows a left ventricular ejection fraction (LVEF) of 40% without segmental wall-motion abnormality. The patient wishes to minimize his medication regimen. What change in his management would you recommend?
Intermittent claudication is characterized by which of the following?
Which of the following deficiencies does not cause dilated cardiomyopathy?
Accelerated Idioventricular Rhythm (AIVR) is the most common arrhythmia associated with:
Which of the following conditions is associated with a giant 'a' wave in the jugular venous pressure?
A patient presents with a new systolic murmur in the left lower sternum following a myocardial infarction. Which of the following is the LEAST likely cause?
Cardiac tamponade is characterized by all of the following except:
Which of the following statements is not true about Brugada syndrome?
A 60-year-old female is undergoing PCI after a coronary narrowing was found on a previous diagnostic angiography. She is known to have coronary vessels prone to spasm. What is the most appropriate management plan when her systolic blood pressure suddenly drops to 70mmHg during the procedure, accompanied by pallor, clamminess, and light-headedness? Her pulse rate is 70bpm and regular.
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app