
Cardiology — MCQs

On this page
Hibernating myocardium is:
Pulsus alternans occurs in which of the following conditions?
A patient with Deep Vein Thrombosis (DVT) on a therapeutic dose of Warfarin presents with complaints of breathlessness and hypotension. Which statement regarding management is true?
Reversible myocardial stunning with ECG changes of acute myocardial infarction is seen in which of the following conditions?
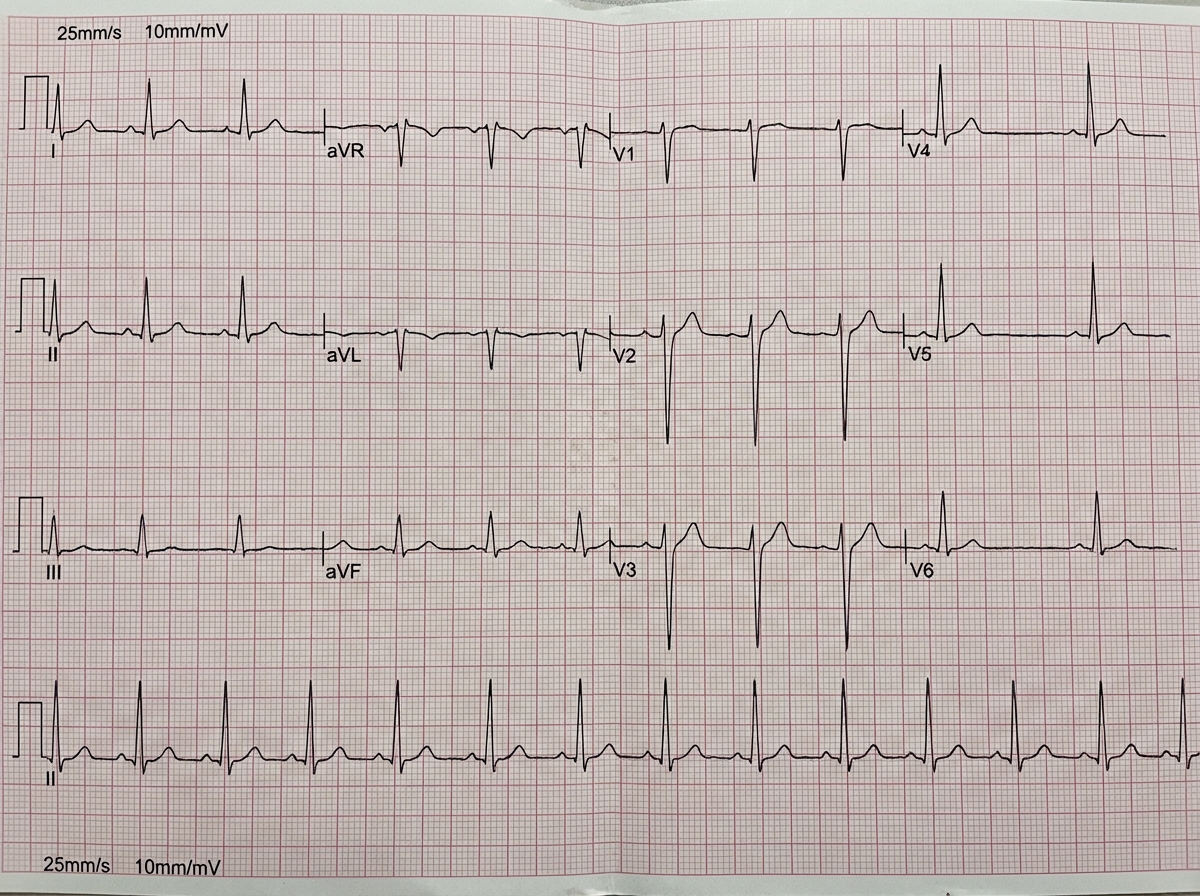
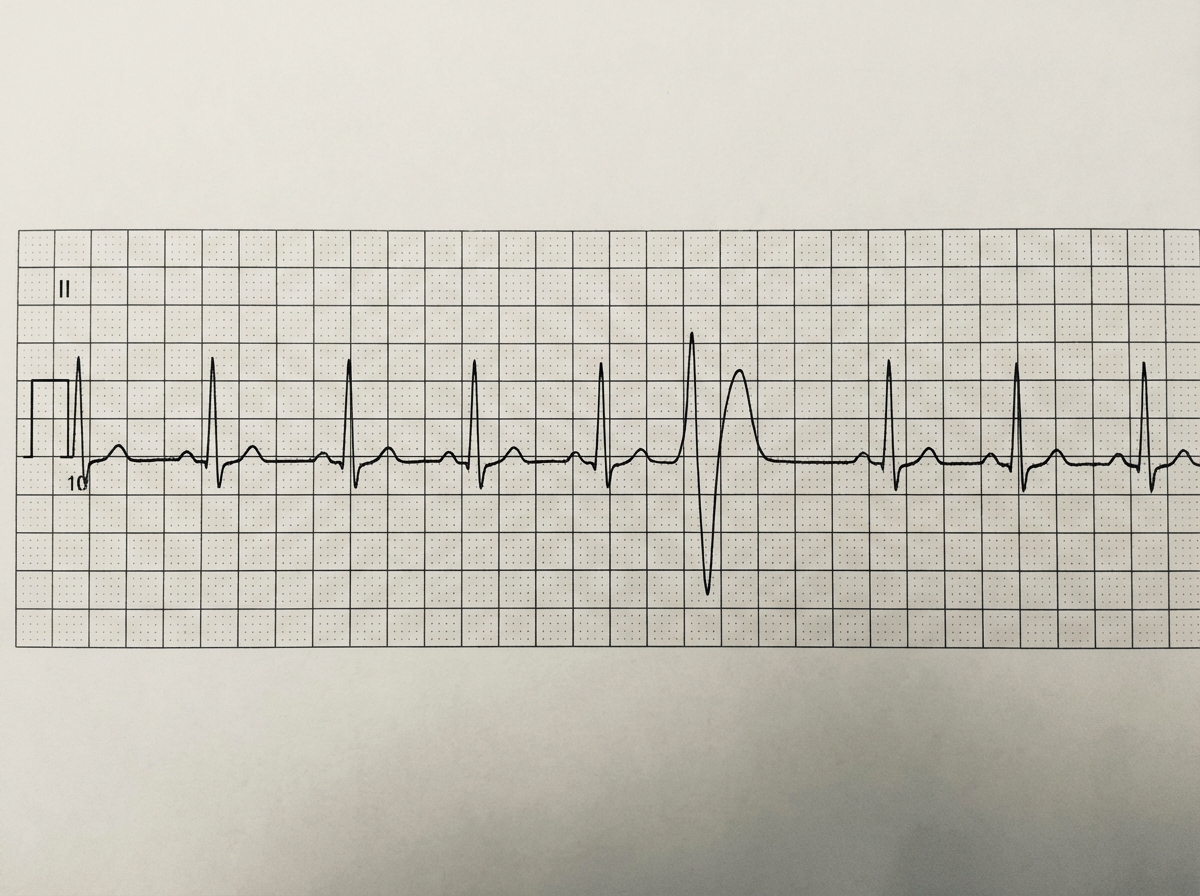
A 35-year-old lady presents with erythema migrans on her trunk following a recent camping trip, along with repeated episodes of syncope on sudden change of position. What does the ECG show?
A 72-year-old man has had poorly controlled hypertension for the past 20 years. Over the past day he has had a severe headache with nausea, followed by confusion, then convulsions. On examination he is afebrile, but his blood pressure is now 260/150 mm Hg. There is bilateral papilledema. Which of the following pathologic lesions is most likely to have developed in his brain during the past day?
What is the most common valvular lesion in carcinoid syndrome?
A 60-year-old man presents with dizziness, nausea, and shortness of breath of several months' duration. Physical examination shows hepatomegaly, ascites, and anasarca. His blood pressure is 200/115 mm Hg. A chest X-ray demonstrates cardiomegaly and mild pulmonary edema. Although different mechanisms may have contributed to the pathogenesis of hypertension in this patient, what is the common end result for all of them?
All are features of the given ECG except:
Which of the following is NOT a feature of atrial septal defect?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app