
Cardiology — MCQs

On this page
A patient with VSD develops pulmonary hypertension. What is the characteristic feature?
A 62-year-old man with carcinoma of the lung presented to the emergency department with respiratory distress. ECG showed electrical alternans. What is the most likely diagnosis?
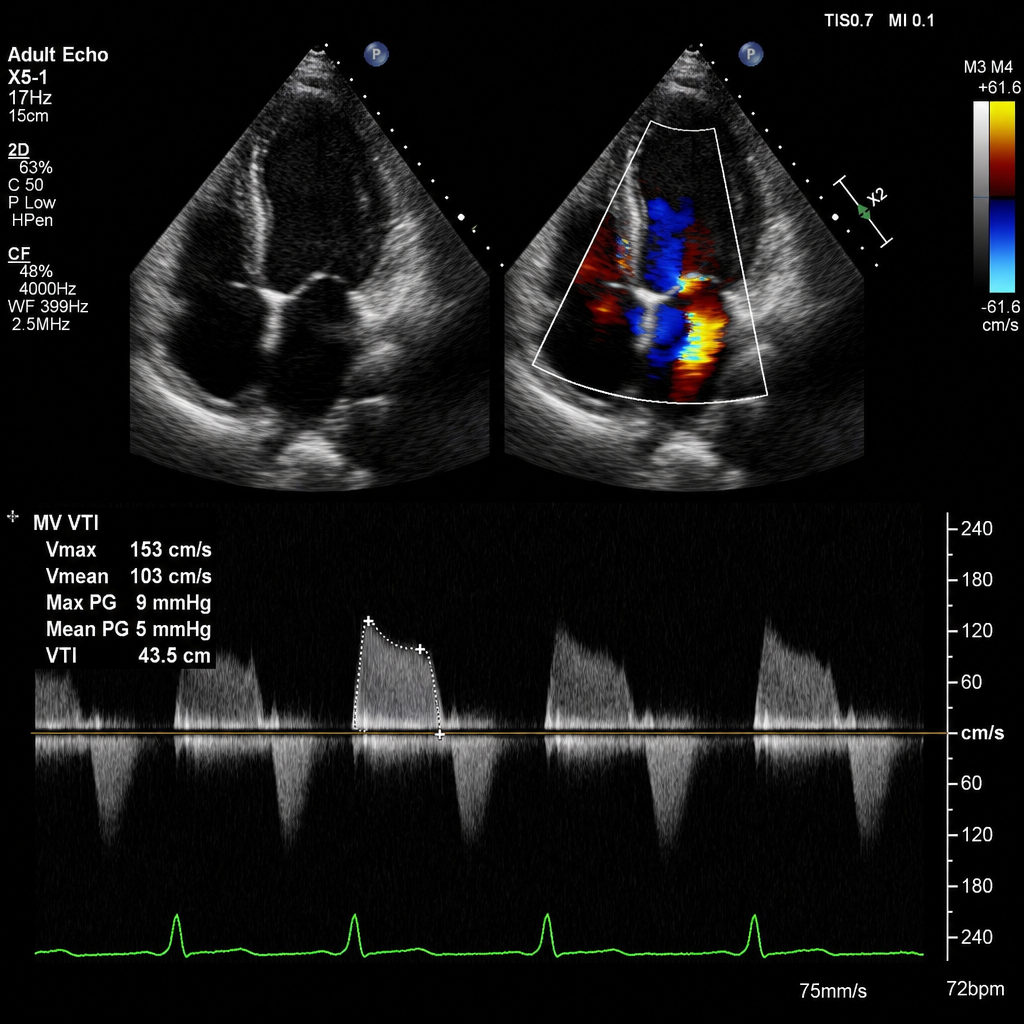
A 58-year-old woman presents for routine cardiac follow-up. Transthoracic echocardiography is performed. Color Doppler imaging shows a mitral regurgitation jet occupying 20–29% of the left atrial area. The vena contracta width measures 0.4 cm. The effective regurgitant orifice area (EROA) is 0.25 cm², and the regurgitant volume is 38 mL. The left atrium is mildly enlarged. Pulmonary vein flow shows blunted systolic filling. There is no evidence of severe left ventricular dilation. What is the severity of mitral regurgitation?
Pulsus paradoxus is not seen in:
What is the treatment of choice in a patient with Wolff-Parkinson-White syndrome and a high-risk accessory pathway?
A patient with a moderate ventricular septal defect (VSD) in chronic congestive heart failure (CCF) develops clubbing without cyanosis. What is the most likely diagnosis?
A 20-year-old man presents for a routine examination. He is afebrile and has clear breath sounds. Cardiac examination reveals a mid to late diastolic murmur, loudest at the cardiac apex. What is the most likely cause of this murmur?
Left axis deviation is seen as?
A 56-year-old African-American man with COPD presents for a routine examination. His average diurnal ambulatory blood pressure is 148/92 mmHg. Laboratory studies show a creatinine level of 3.2 mg/dL and a potassium level of 5.6 mg/dL. Which of the following medications would most likely be considered the first-line treatment in this patient?
What happens to the Austin Flint murmur after exposure to vasodilators?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app