
Cardiology — MCQs

On this page
A 40-year-old woman presents with a 3-year history of increasing dyspnea and fatigue. Physical examination reveals increased jugular venous pressure with prominent c-v waves, a reduced carotid pulse, a left parasternal lift, loud P2, and right-sided S3 and S4 gallops. Lung fields are clear on chest X-ray, and ECG shows evidence of right ventricular hypertrophy. Pulmonary function tests show a slight restrictive pattern. Primary pulmonary hypertension is suspected. Which of the following is the most appropriate diagnostic test to confirm the diagnosis?
RBBB with left axis deviation is characteristic of which condition?
A 42-year-old smoker has developed an acute anterior wall myocardial infarction. Which of the following coronary arteries is most likely to show obstruction?
Water hammer pulse is seen in which of the following conditions?
Which of the following increases susceptibility to coronary artery disease?
Which of the following is not a first-line antihypertensive medication?
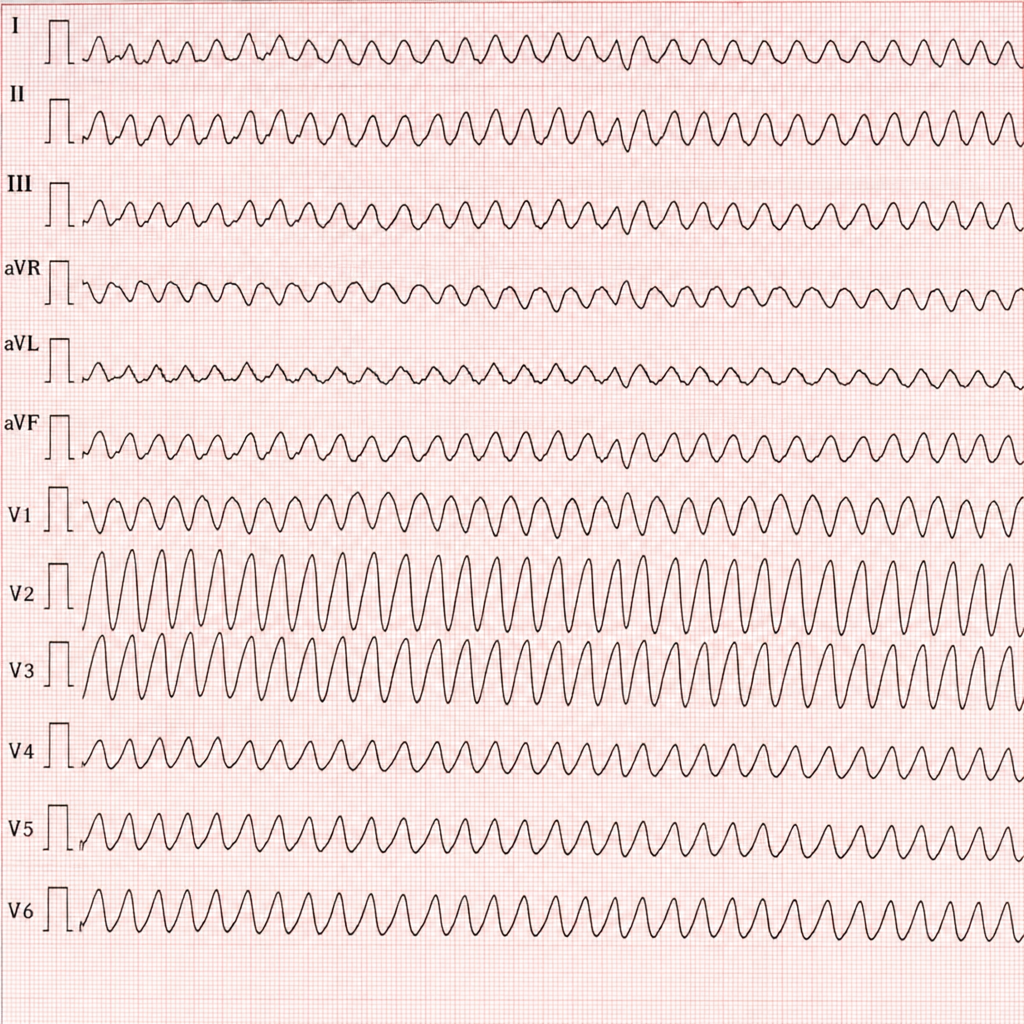
A 70-year-old male with a history of hypertension and diabetes mellitus developed the following rhythm with a blood pressure of 90/40 mm Hg and a feeble pulse. What is the next step in management?
Which of the following is NOT a feature of ventricular tachycardia?
All of the following auscultatory findings are heard in chronic mitral stenosis except?
Which of the following conditions is NOT associated with long and peaked 'a' waves in the jugular venous pulse waveform?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app