
Cardiology — MCQs

On this page
Recurrent ischemic events following thrombolysis have been pathophysiologically linked to which of the following factors?
What is the level of LDL cholesterol at which therapy should be initiated in a patient without coronary artery disease and no risk factors?
A 55-year-old woman with a recent diagnosis of amyloidosis presents with increasing shortness of breath, fatigue, and edema. Examination reveals a JVP of 10 cm with prominent x and y descents but a negative Kussmaul's sign. Her blood pressure is 90/70 mm Hg, pulse is 100/min with low volume, and there is no pulsus paradoxus or abnormal heart sounds. What is the most likely diagnosis for this patient presenting with shortness of breath and peripheral edema?
Ventricular aneurysm has one of the following characteristic features?
A patient presented with pulsating varicose veins of the lower limb. What is the most probable diagnosis?
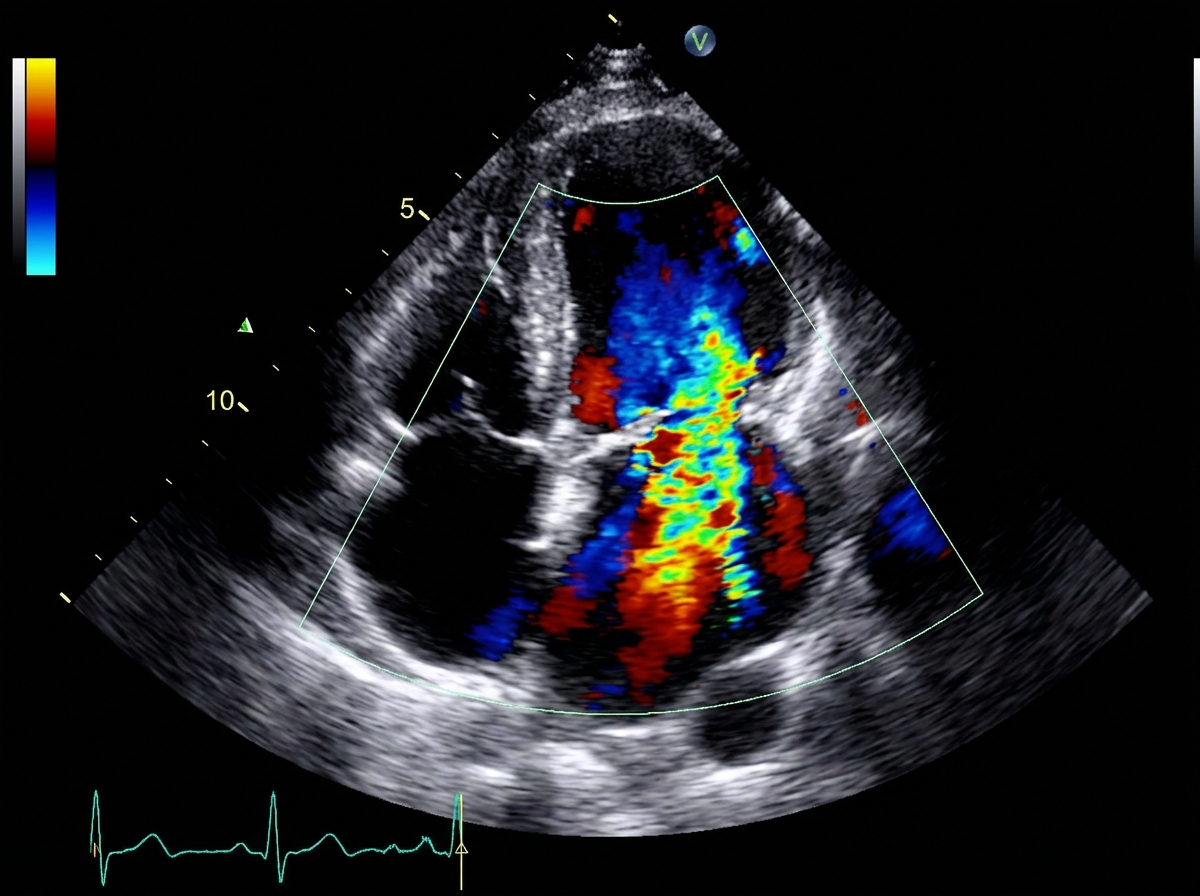
A patient undergoes echocardiographic evaluation. The color Doppler image below is obtained. Additional quantitative Doppler measurements reveal a vena contracta width of 0.8 cm, EROA of 0.45 cm², regurgitant volume of 65 mL, regurgitant fraction of 55%, and systolic pulmonary vein flow reversal. What is the severity of mitral regurgitation (MR)?
A 45-year-old smoker presents with sudden onset unrelenting chest pain and loss of peripheral pulses. Blood pressure measured in both arms is different. What is the most likely first differential diagnosis?
Paradoxical embolism is detected by?
Which congenital heart disease is associated with pre-excitation?
A 70-year-old man presents with isolated systolic hypertension. His blood pressure is 170/80 mm Hg, and physical examination reveals normal heart and lungs. He has no other medical conditions. For a patient with high blood pressure, select the most appropriate medication.
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app