
Cardiology — MCQs

On this page
A 48-year-old male presents with a history of precordial chest pain. His blood pressure is 80/60 mm Hg. An ECG shows a wide QRS complex with no preceding P waves and a rate of 112/min. What is the most immediate step in the management of this patient?
A 65-year-old man presents with dyspnea, chest pain, and several syncopal episodes. His symptoms have worsened over the past few months, and his third syncopal episode prompted this visit. On examination, a systolic ejection murmur with an ejection click is auscultated in the right second intercostal space. Rales are present at the lung bases. He has a history of rheumatic fever in his twenties. Which of the following might explain the angina pectoris in this patient?
Which of the following is NOT associated with prolonged QT syndrome?
What is the metabolic defect in accelerated hypertension?
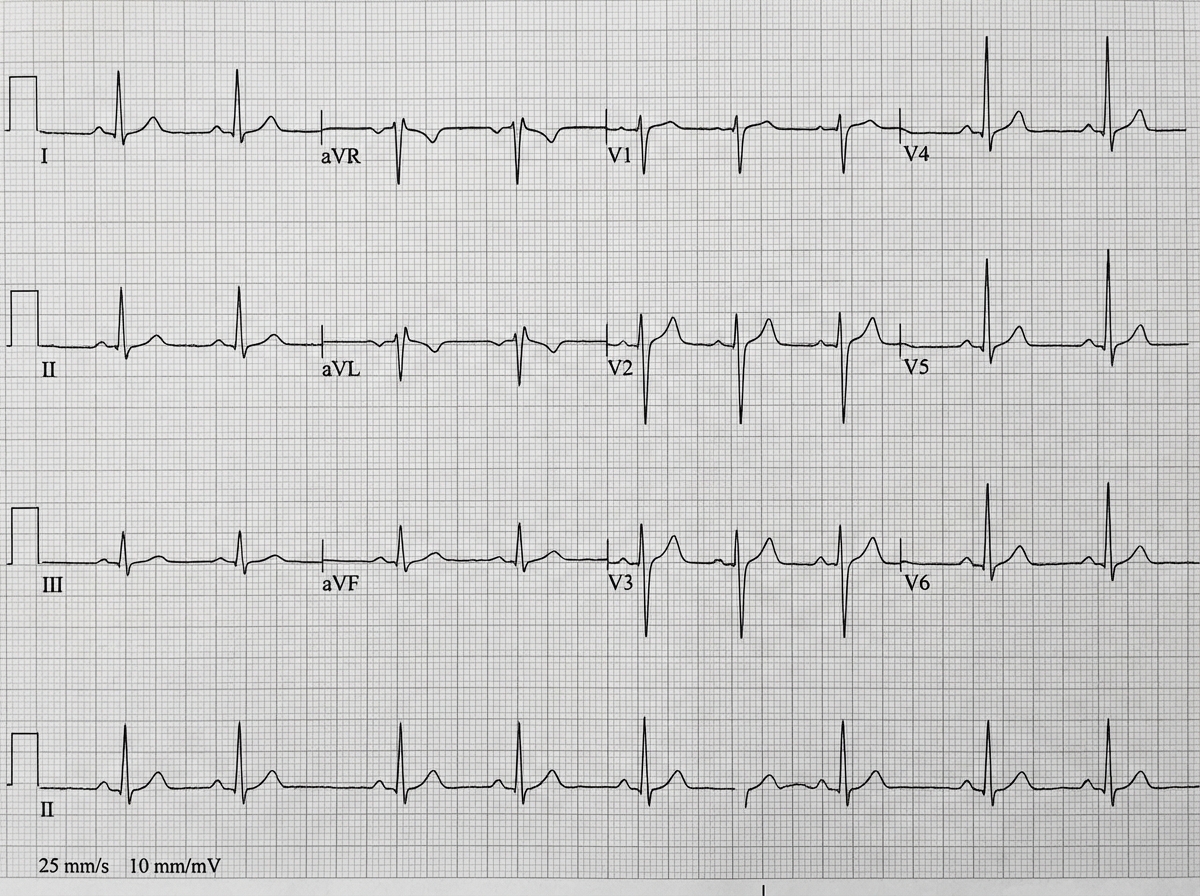
A 72-year-old male presented to the ER with falls. Based on the provided ECG interpretation, what is the likely diagnosis?
What is the characteristic cardiac anomaly associated with Lutembacher syndrome?
Pulsus paradoxus is seen in which of the following conditions?
Which of the following is seen in torsades de pointes?
A 20-year-old female patient presents with non-exertional chest pain. On auscultation, she has multiple non-ejection clicks. What is the investigation of choice?
A 23-year-old male presented with excruciating chest pain and palpitations after consuming multiple energy drinks. His ECG showed sinus tachycardia but no ST changes. His pulse was 90/min and BP was 130/90 mm Hg. The pain subsided shortly after. His physical examination was normal. He reported that his father had a myocardial infarction at the age of 60. All laboratory findings, including troponin and D-dimer tests, were within normal ranges. What should be the next step in management?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app