
Cardiology — MCQs

On this page
Which of the following differentiates ventricular tachycardia from Wolff-Parkinson-White (WPW) pattern with atrial fibrillation?
A 41-year-old woman presents with chest pain, shortness of breath, and worsening fatigue for the past day. The chest pain initially worsened with lying down and improved with leaning forward, but now it seems equal in intensity over all positions. On examination, she has labored, fast breathing and appears to be in pain. She has jugular venous distention. She is tachycardic, and has distant heart sounds with a friction rub. Her lungs are clear to auscultation bilaterally, and she has no limb edema. Her pulse is 126/min, BP is 89/66 mm Hg, respiratory rate is 32/min, and oxygen saturation is 98% on room air. Which of the following is the most likely diagnosis?
Which of the following statements regarding the ECG findings in acute pericarditis is FALSE?
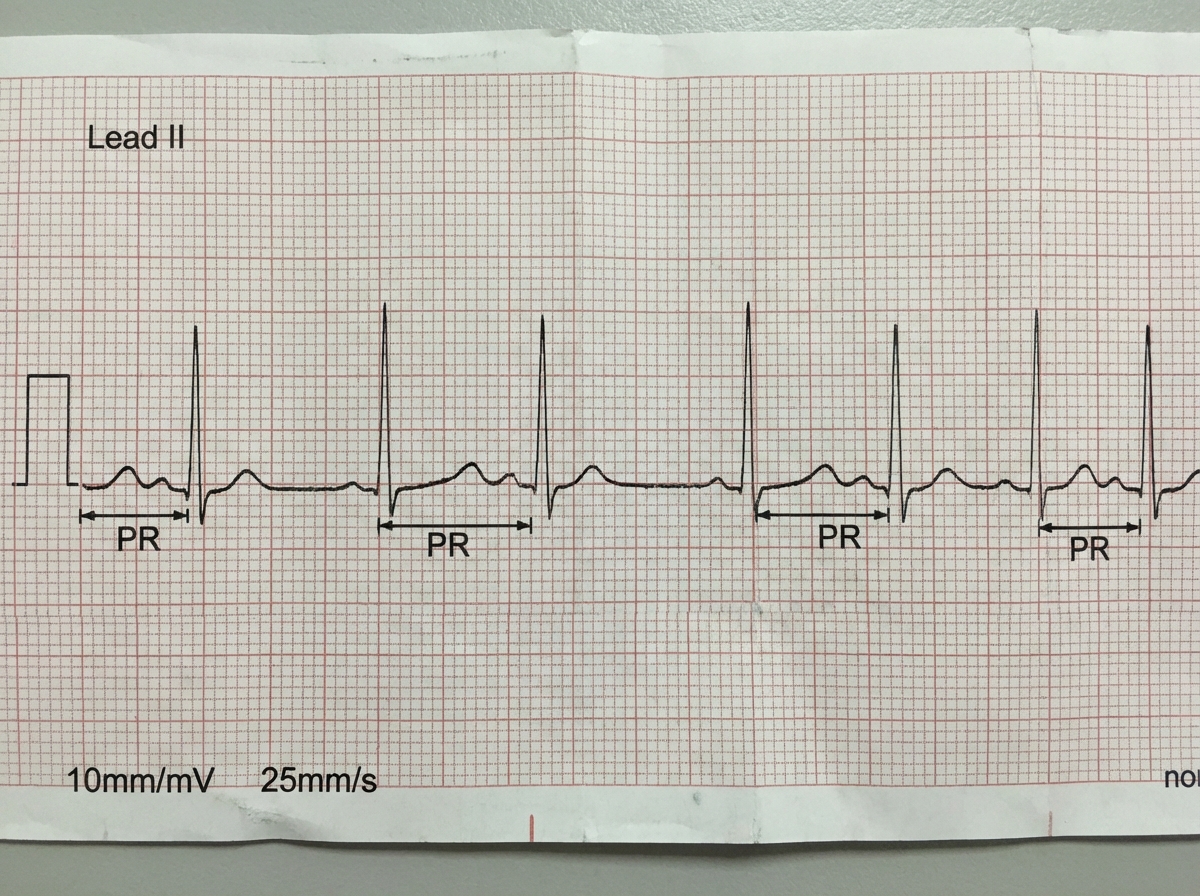
What does the ECG show?
What type of mutation is most commonly associated with Brugada syndrome?
Pulse deficit may be seen in all of the following, except:
A dicrotic pulse is observed in which condition?
What is the most common cause of mitral stenosis?
What is the drug of choice for persistent unstable ventricular arrhythmia?
Pseudo resistant hypertension is seen in which situation?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app