
Cardiology — MCQs

On this page
A patient presents with shortness of breath. On clinical examination, he is found to have a heaving apex and a systolic murmur that intensifies on Valsalva's maneuver. What is the most likely diagnosis?
In atrial septal defect, what is the typical size of the aorta?
Diagnosis of tubercular pericarditis can be done by:
Blunted 'y' descent is seen with which of the following conditions?
Which of the following is a cause of wide pulse pressure?
What is the most common cause of hypertension in a 45-year-old male with a 20-year history of smoking?
Total electrical alternans in ECG along with sinus tachycardia is a specific sign of which condition?
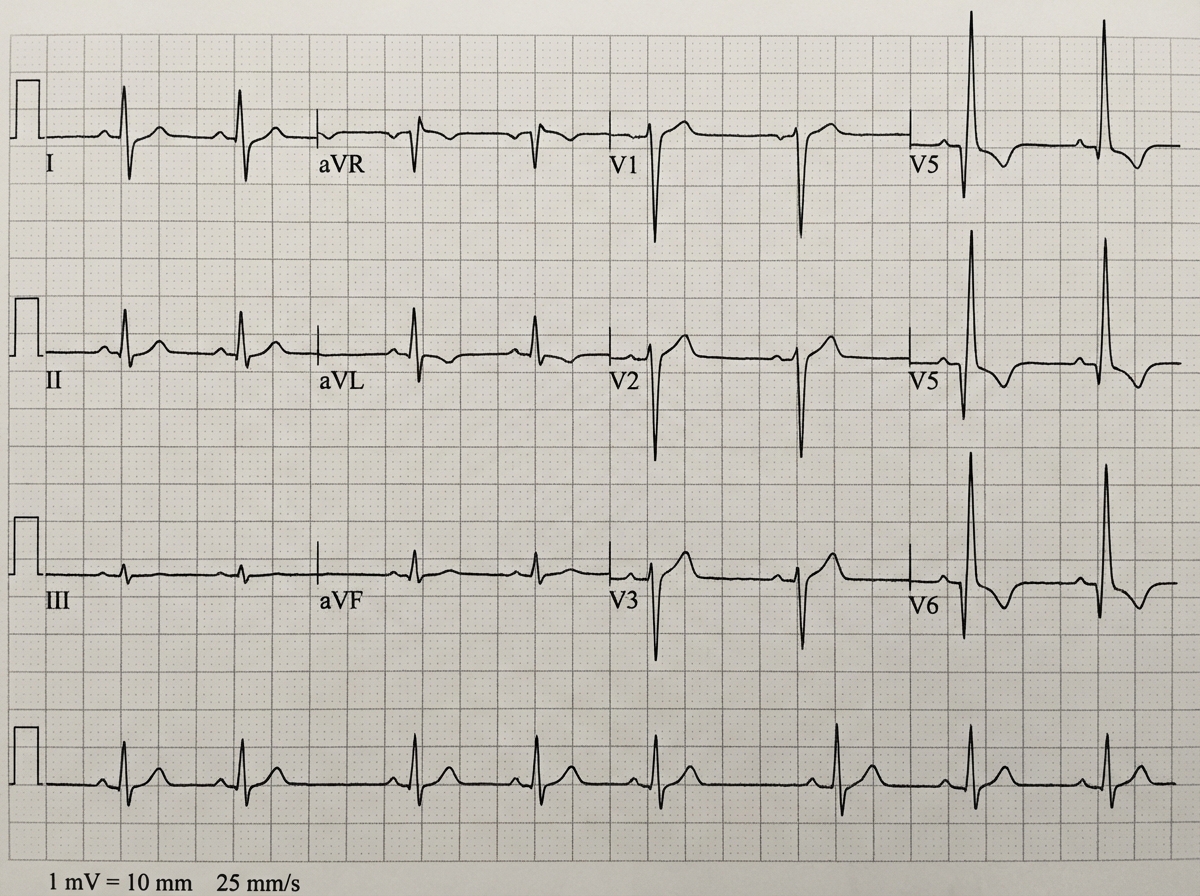
An 18-year-old male presents with loss of consciousness during exertion. He regained consciousness fully in the ER, with a GCS of 15/15 on admission. His neurological examination is normal. On auscultation, a narrow split S2, a dynamic systolic murmur that increases with Valsalva, and clear lungs are noted. An ECG was performed. What is the most likely diagnosis?
Which of the following is NOT a feature of acute pericarditis?
A 22-year-old woman complains of palpitations and has a regular heartbeat at a rate of 170/min, with a blood pressure of 110/70 mm Hg. The rate abruptly changes to 75/min after applying carotid sinus pressure. Which of the following is the most likely diagnosis?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app