
Cardiology — MCQs

On this page
Which type of cardiomyopathy is typically seen in individuals with chronic alcoholism?
An otherwise healthy athlete complains of chest pain and dyspnea during routine training, has a double impulse at the apex on examination, and undergoes sudden death. What is the likely diagnosis?
An elderly man with known ischemic heart disease develops syncope. Peripheral pulses are absent, blood pressure is not recordable, and ECG reveals wide complex tachycardia. What is the immediate management?
The 'a' wave in JVP is seen in which of the following conditions?
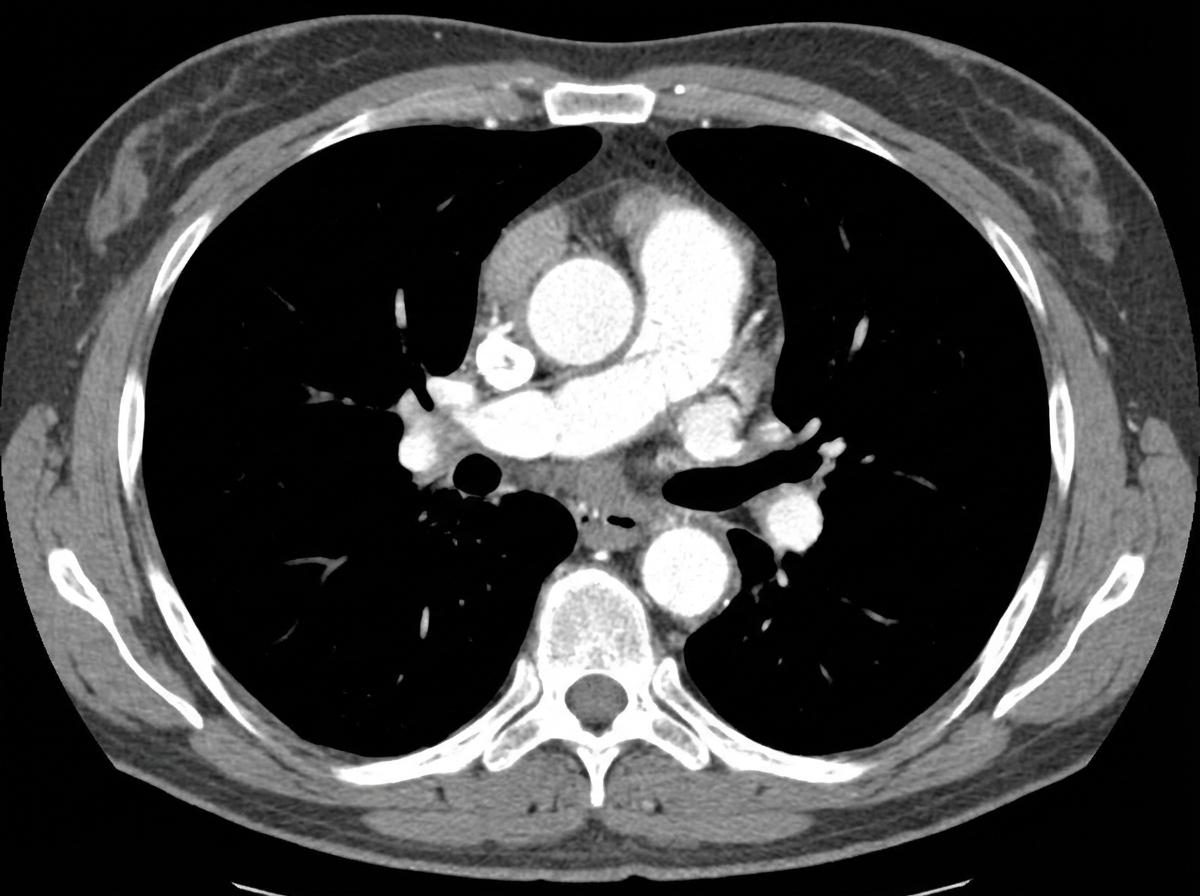
A 50-year-old male presented to the emergency department with a blood pressure of 160/100 mmHg and a heart rate of 120 bpm. A CECT scan was performed, and the image is provided. What is the management of the condition shown?
A patient presents with palpitations. He has no past history of similar episodes but reports consuming a large amount of coffee at work. What is the most appropriate first-line treatment for this patient?
A 26-year-old asymptomatic woman is found to have arrhythmias and a systolic murmur associated with midsystolic clicks. Which investigation would you use?
An 84-year-old man with a history of smoking and a myocardial infarction 2 years ago presents with chest and leg pain during exercise. His vital signs are temperature, 37.1°C; pulse, 81/min; respirations, 15/min; and blood pressure, 165/100 mm Hg. Peripheral pulses are diminished in the lower extremities. A 7-cm pulsating mass is palpable in the midline of the lower abdomen. Laboratory studies show fasting serum glucose levels of 170 mg/dL and 200 mg/dL. Which of the following vascular lesions is most likely to be present in this patient?
Which of the following drugs is contraindicated for the treatment of atrial fibrillation associated with Wolff-Parkinson-White (WPW) syndrome?
Cannon 'a' waves in the venous waveform are suggestive of what condition?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app