
Cardiology — MCQs

On this page
Low renin hypertension is seen in all of the following conditions, except:
Acute aortic regurgitation is seen in all the following conditions except?
In Myocardial infarction, what is the most specific marker?
Which of the following is untrue regarding sick sinus syndrome?
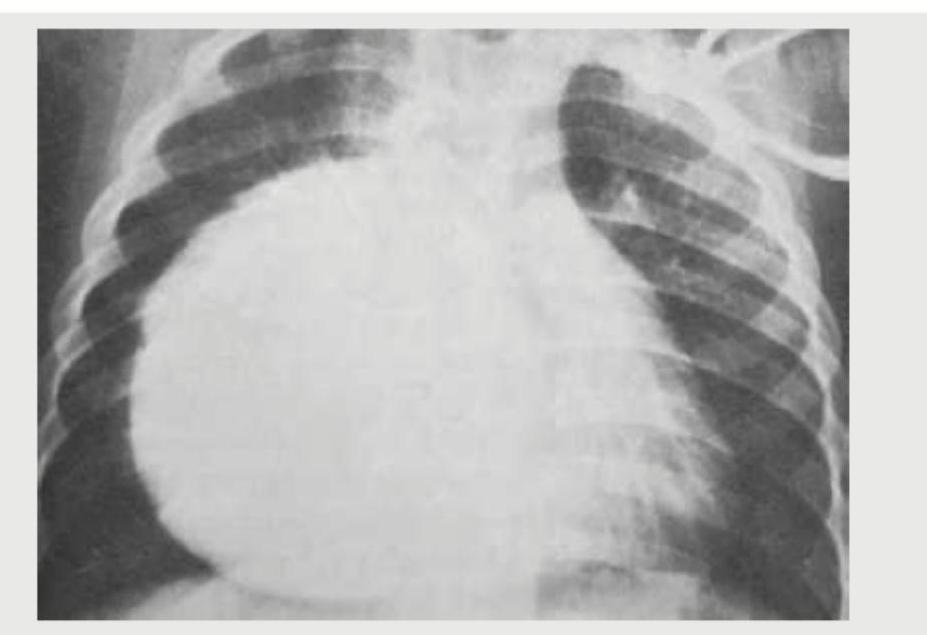
A 60-year-old smoker presents with breathlessness for 2 weeks. On examination, heart rate is 100/min, BP = 90/60 mm Hg, and neck veins are distended with a palpable liver. CXR is shown. What is the probable diagnosis?
Regarding Hypertrophic Obstructive Cardiomyopathy (HOCM), all are true except?
What is the critical degree of narrowing of coronary vessels that causes angina?
Giant 'a' waves in JVP occur in all except?
A 49-year-old man has his serum lipids measured. Which pattern suggests the lowest risk for coronary artery disease?
The murmur of hypertrophic cardiomyopathy is decreased in which of the following positions or maneuvers?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app