
Cardiology — MCQs

On this page
A 40-year-old man with a history of intravenous drug abuse develops rapidly progressive right-sided heart failure. Which of the following conditions is the most likely cause?
N-terminal pro-brain natriuretic peptide (NT-proBNP) levels are elevated in which of the following conditions?
Asynchronous cardioversion is indicated in which of the following arrhythmias?
A 36-year-old female presents with recurrent chest pain and palpitations of varying duration and severity, with 6-7 ectopic beats per minute. These symptoms are not related to exertion. Her blood pressure is 86 mm Hg and pulse rate is 86/min. What is the ideal investigation?
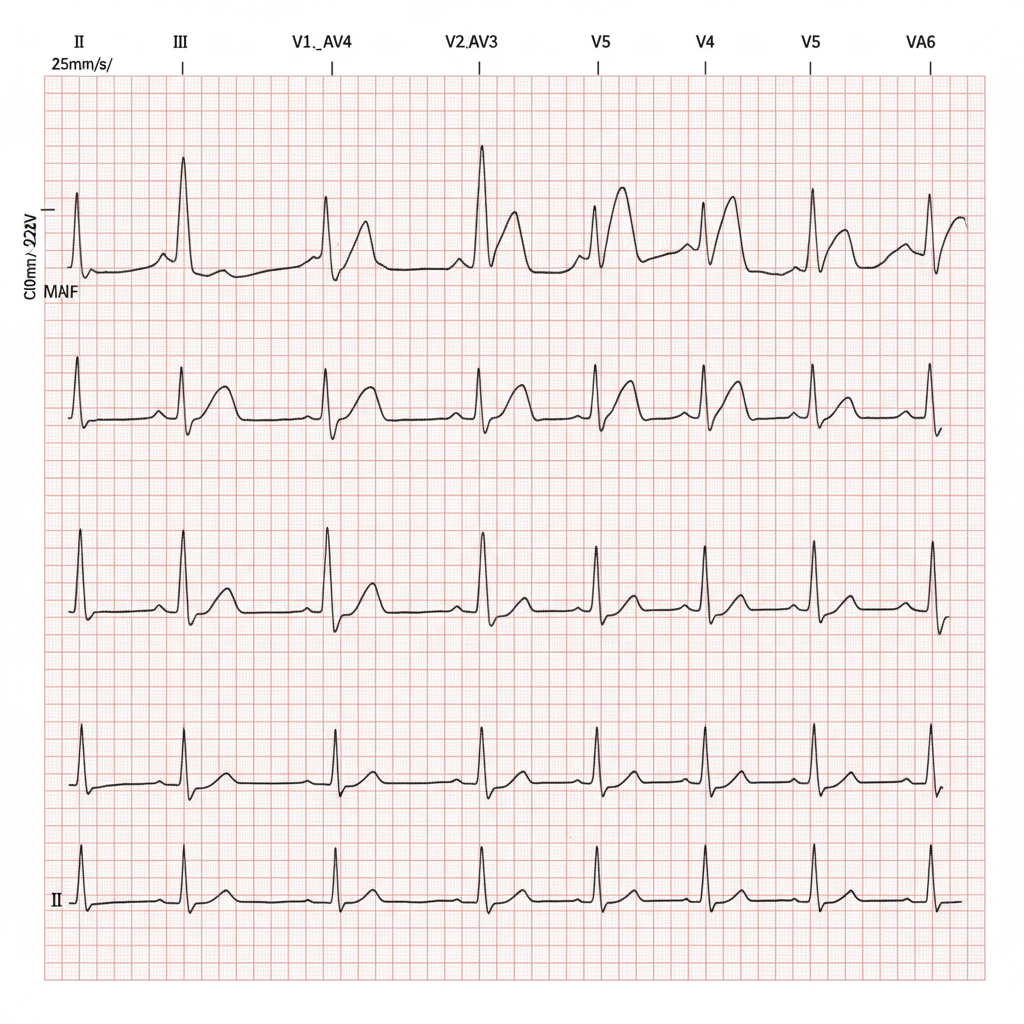
A 70-year-old woman with known diabetes mellitus presents with dyspnea, nausea, and a feeling of impending doom. What does the ECG show?
Lambert-Eaton myasthenic syndrome is associated with which of the following?
A patient presents with ventricular fibrillation, hypotension, and absent peripheral pulses. What is the initial management?
A 60-year-old man with a history of left ventricular aneurysm post-myocardial infarction in 2017 presents with recurrent episodes of syncope. Following consumption of coffee, he experienced syncope and was brought to the hospital. What is the best management strategy to prevent future episodes?
Severe hypertension is defined if systolic BP is greater than:
In the JVP tracing, which condition is characterized by the absence of 'a' waves?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app