
Cardiology — MCQs

On this page
A 46-year-old diabetic man complains of soreness of the left leg. He is moderately obese and had undergone cholecystectomy 2 weeks ago. Examination revealed swelling in the lower leg along with tenderness in the calf that increased when the calf was gently squeezed. No redness of the leg was noted and the patient was afebrile. What is the most likely diagnosis?
Which of the following statements regarding torsades de pointes is FALSE?
Osler's nodes are seen at:
Non-ejection clicks are heard in which of the following conditions?
Women with myocardial infarction are more likely to present with which of the following complications than males?
Changing character of a murmur in a patient with joint pain and embolic phenomenon indicates which of the following diagnoses?
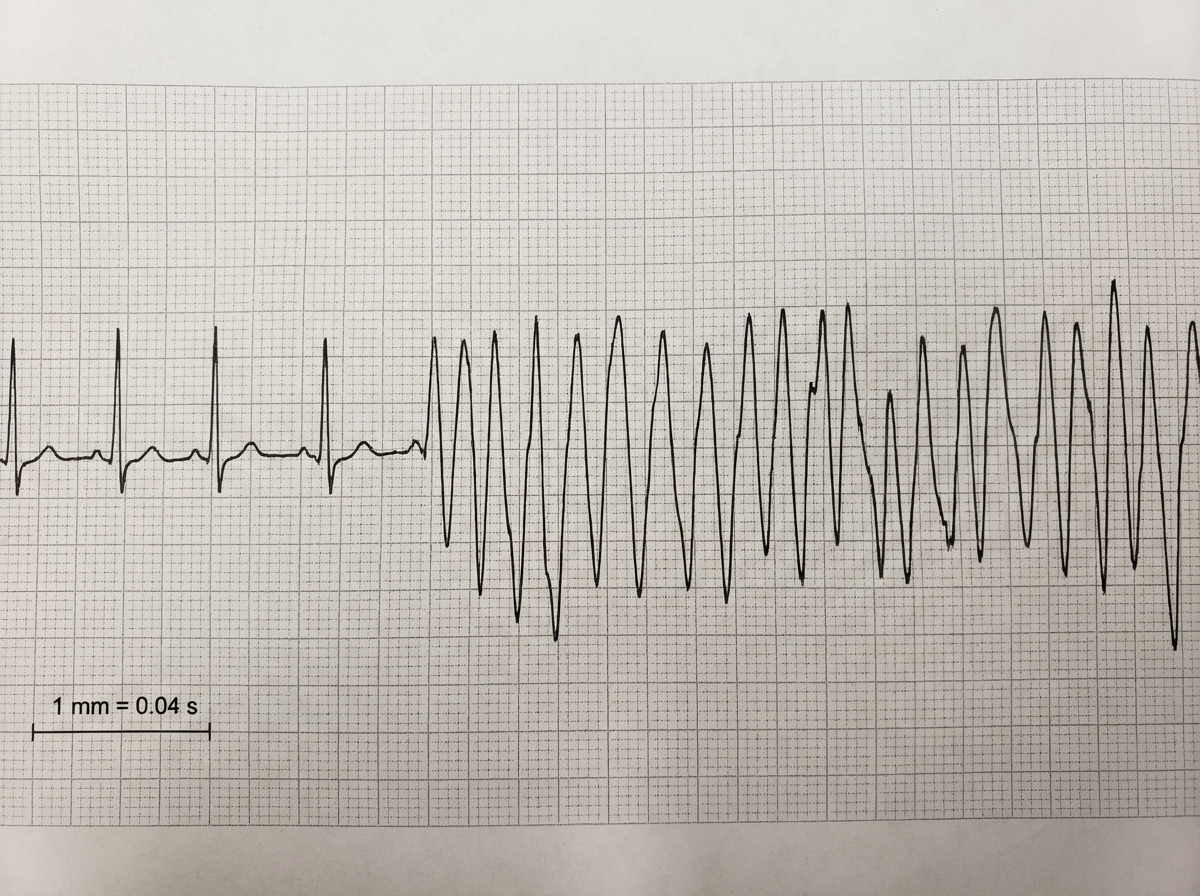
All the following statements are true regarding the given ECG except?
A 45-year-old man experiences crushing substernal chest pain after arriving at work one morning. Over the next 4 hours, the pain persists and begins to radiate to his left arm. He becomes diaphoretic and short of breath but waits until the end of his 8-hour shift to go to the hospital. An elevated serum value of which of the following laboratory tests would be most useful for the diagnosis of this patient on admission to the hospital?
Which of the following is NOT true regarding Mitral valve prolapse syndrome?
A 64-year-old man with a history of COPD presents with increased shortness of breath, cough, and sputum production, but no fever or chills. On examination, he is in mild respiratory distress with a respiratory rate of 26/min, pulse of 120 beats/min, blood pressure of 145/84 mm Hg, and oxygen saturation of 90%. He has bilateral expiratory wheezes. His ECG reveals multifocal atrial tachycardia (MAT), characterized by discrete P waves with at least three different morphologies. What is the most appropriate treatment for this patient's arrhythmia?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app