
Cardiology — MCQs

On this page
All the following are features of constrictive pericarditis except?
Which of the following conditions exhibits increased murmur intensity upon standing?
Which of the following is the earliest cardiac abnormality to develop in acute rheumatic fever?
A 63-year-old woman presents with symptoms of palpitations and atrial flutter on the ECG. Which of the following is the most likely mechanism of this arrhythmia?
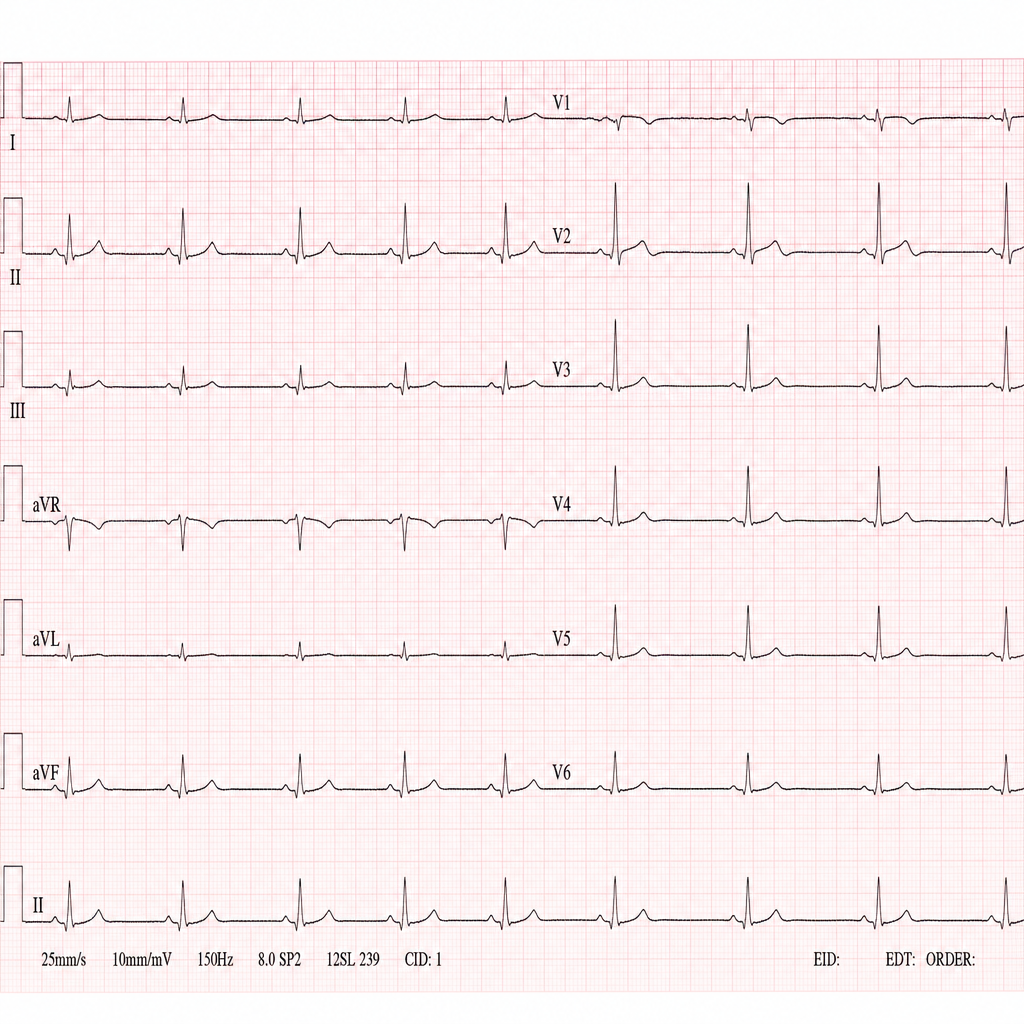
A 70-year-old woman had an ECG at her annual checkup. Calculate her heart rate using the lead II recording.
Intracavitary electrocardiography is a diagnostic aid in?
What medication is indicated for a 62-year-old hypertensive patient with high lipids and atherosclerosis?
A 47-year-old woman presents with new-onset transient right arm weakness and word-finding difficulty lasting 3 hours. She also experiences exertional dyspnea and had a syncopal event 1 month ago. Her medical history is remarkable only for 2 uneventful pregnancies, and she is not taking any medications. Physical examination reveals normal vital signs and no residual focal neurological deficits. The ECG and CT brain are normal, but an echocardiogram reveals a cardiac tumor in the left atrium, which is pedunculated and attached to the endocardium. Which of the following is the most likely cause of this lesion?
Which of the following is NOT a cause of Pulseless Electrical Activity (PEA)?
What is the effect of beriberi on circulation?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app