
Cardiology — MCQs

On this page
Which of the following ECG changes is NOT typically seen in hyperkalemia?
A 58-year-old man had a myocardial infarction 1 year ago. He now wants to prevent another acute coronary event and is advised to begin a program of exercise and to change his diet. A reduction in the level of which of the following serum laboratory findings 1 year later would best indicate the success of his diet and exercise regimen?
Stokes-Adams syndrome is associated with which of the following conditions?
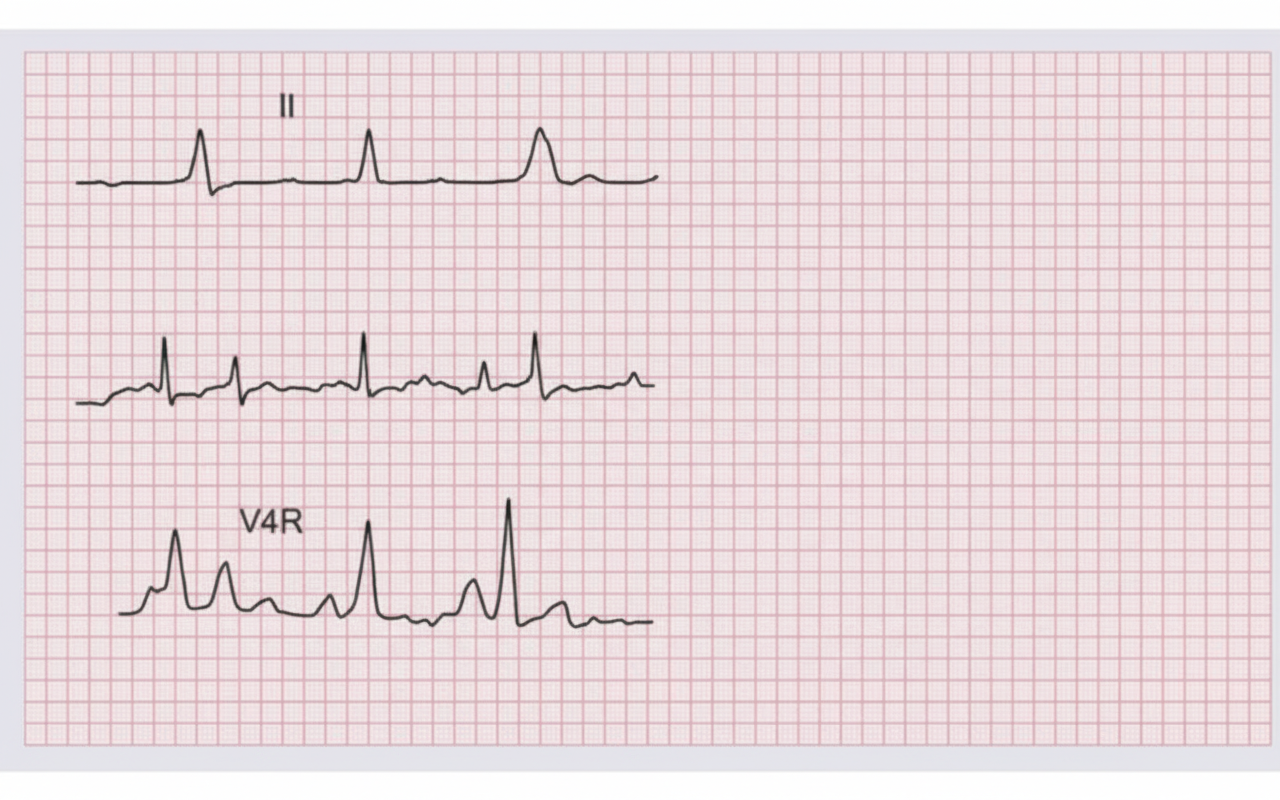
A 65-year old man presents with crushing chest pain for 2 hours. On examination, BP = 80/60 mm Hg and JVP are elevated 6 cm above the sternal angle. All are true about the condition shown except?
What is the treatment of choice for ST-elevation myocardial infarction?
A 38-year-old male presents with a two-week history of progressive shortness of breath. He has a past medical history of type II diabetes mellitus. An echocardiogram revealed an ejection fraction (EF) of 25% with anterior, septal, and lateral wall motion defects. He was admitted and stabilized on furosemide, spironolactone, bisoprolol, and ramipril. What would be the next investigation in the course of management?
Which of the following drugs should not be used empirically in a patient with severe hypertension, especially in the elderly?
Which of the following EKG findings are characteristic of ventricular premature beats?
Which of the following is the first-line vasopressor in the management of cardiogenic shock?
A 50-year-old man had an attack of myocardial infarction and developed ventricular ectopics and a low ejection fraction. Which of the following antiarrhythmic drugs should be given?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app