
Cardiology — MCQs

On this page
An asymptomatic 19-year-old female student presents for routine follow-up. Echocardiogram shows congenital mitral regurgitation. What are the most typical clinical and auscultation findings?
Which of the following heart diseases is the most common cause of sudden death in young athletes?
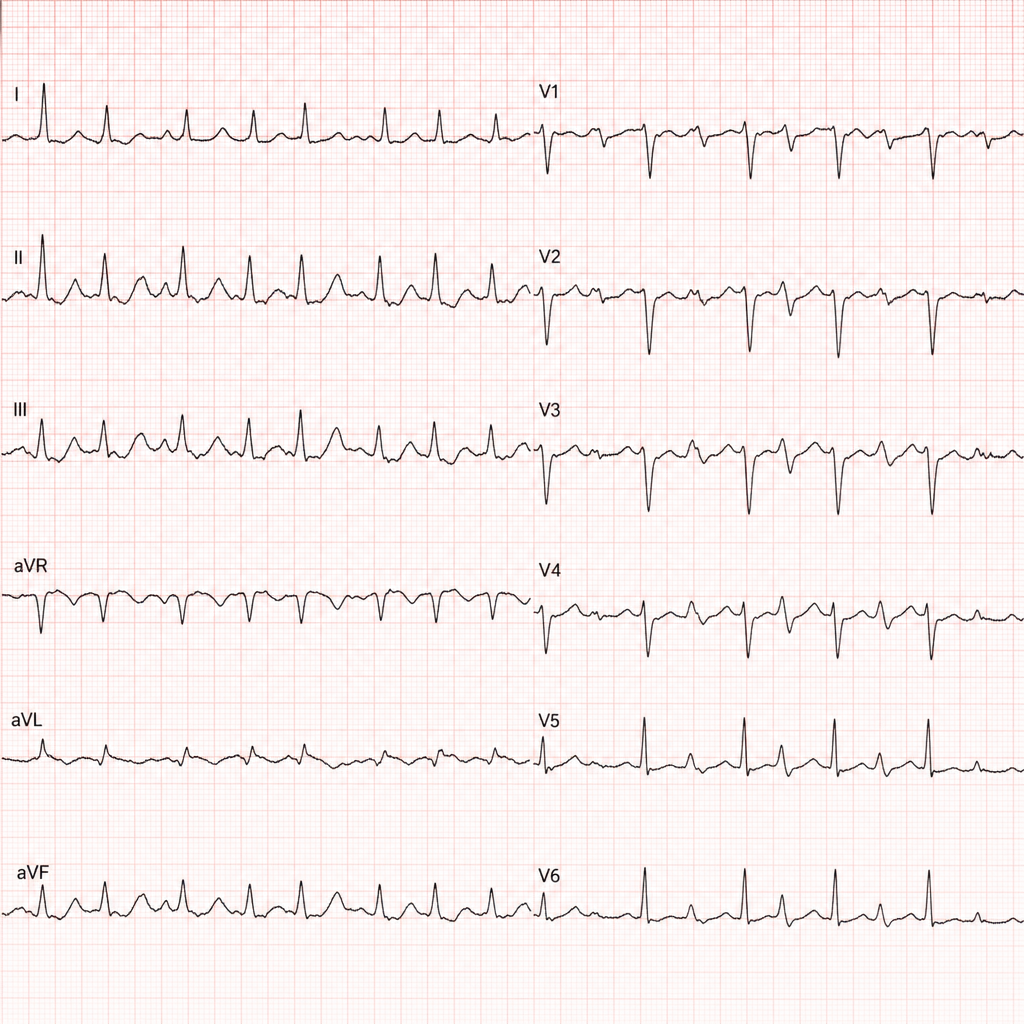
A patient presents with recent onset of breathlessness. An ECG is taken. What is the diagnosis?
What is characteristic of unstable angina?
A 40-year-old male with a tense personality, who suffered from attacks of chest pain diagnosed as angina pectoris, presents with a resting heart rate of 96/min and blood pressure of 170/104 mm Hg. His blood sugar level and lipid profile are normal. Which antihypertensive medication is most suitable for initial therapy in this case?
In ECG leads II, III, and aVF, abnormalities are noted. Which of the following vessels is most likely blocked?
Cardiomyopathy may be seen in all of the following conditions except?
Angiotensin converting enzyme inhibitors are not used in congestive heart failure resulting from which of the following conditions?
In Valvular Aortic Stenosis, when is the prognosis poorest?
A patient presents with an ECG showing ST elevation and low blood pressure. What is the best immediate management?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app