
Cardiology — MCQs

On this page
A systolic thrill in the left 2nd and 3rd intercostal space may be seen in all of the following conditions, except?
All of the following are true about Right Ventricular Infarcts, except?
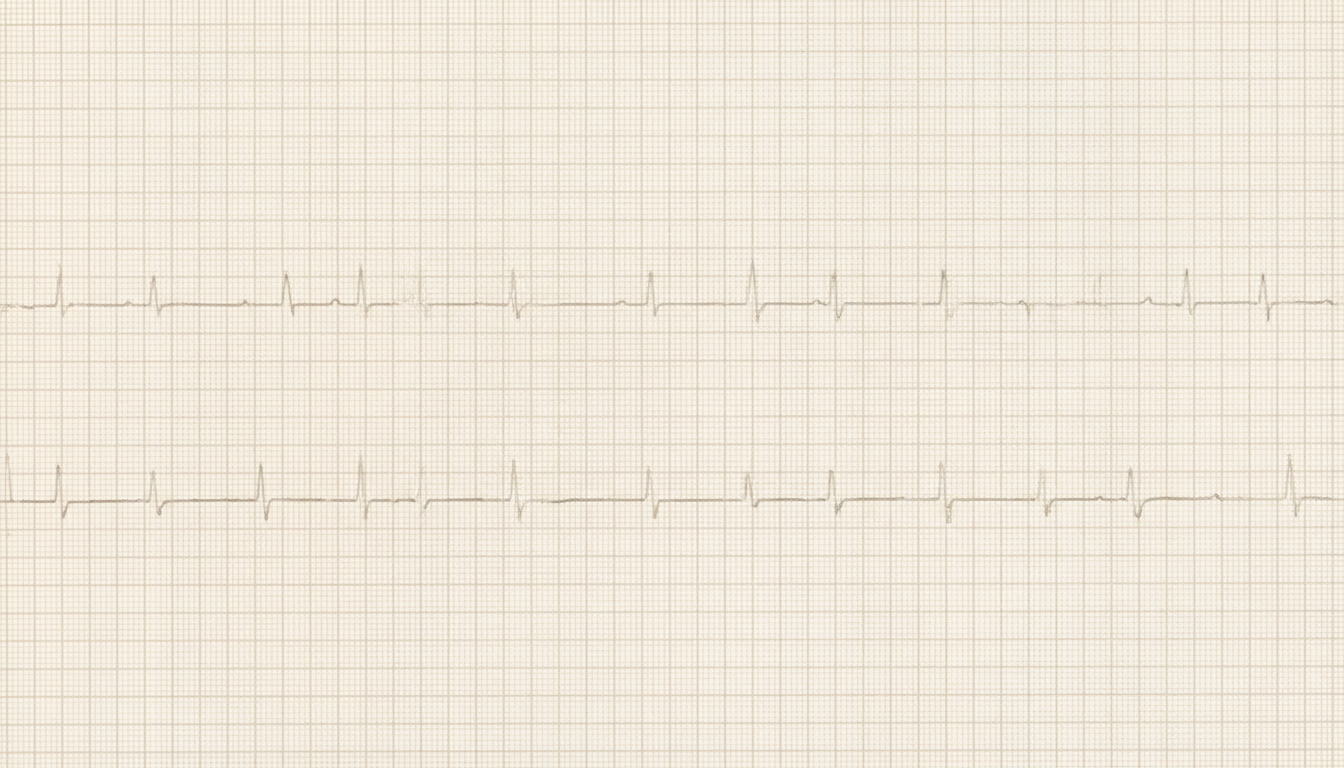
A 68-year-old woman presents to the emergency department complaining of chest pain for the past 30 minutes. The pain is retrosternal in location and it radiates to her neck. She has no history of cardiac conditions or similar episodes of chest discomfort, and her past medical history includes hypertension and dyslipidemia. On physical examination, she is diaphoretic and in moderate distress. The blood pressure is 150/90 mm Hg, the heart sounds are normal, and the lungs are clear on auscultation. The ECG is shown in Figure below. Which of the following mechanisms is the most likely cause of her condition?
Eight days after undergoing a hysterectomy, a 64-year-old woman complains of chest pain. After 12 hours, which test will most likely support the diagnosis of myocardial infarction?
Antibiotic prophylaxis is mandatory before dental extraction in patients with which of the following cardiac conditions?
True about coarctation of aorta?
Which of the following murmurs increases with the Valsalva maneuver?
Sukhia Rani, a 16-year old girl, presents with non-pitting edema of recent onset affecting her right leg and no other symptoms. Which of the following statements is true regarding this patient?
A 16-year-old male is referred for a physical examination before joining the football team. His elder brother died suddenly during football practice; no autopsy was performed. The patient has a loud systolic murmur on chest auscultation. Which of the following findings is inconsistent with hypertrophic cardiomyopathy?
Prolonged QT interval is not seen in which of the following conditions?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app