
Cardiology — MCQs

On this page
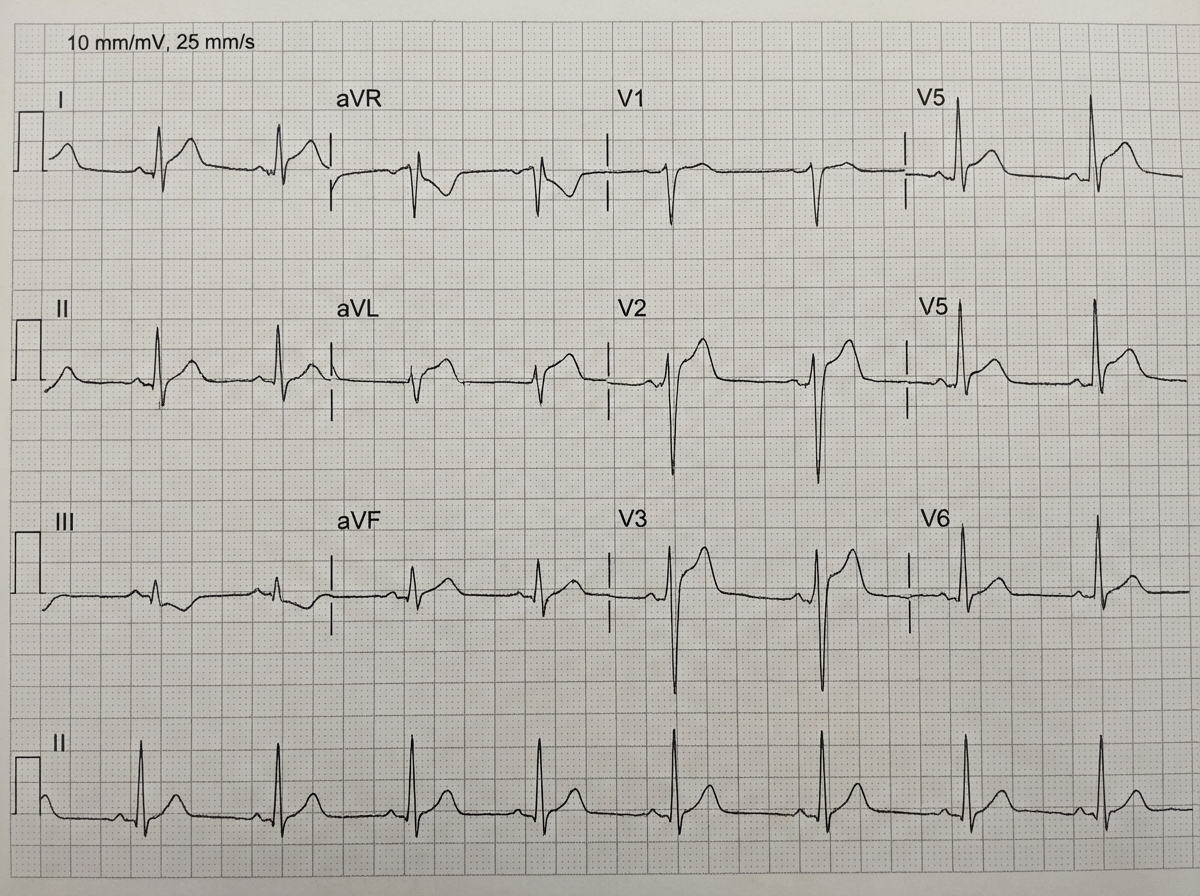
An 89-year-old man with hypertension presents for routine follow-up. What is the primary conduction abnormality seen on this ECG?
Which valvular lesion is being repaired in a 20-year-old man presenting with a malar flush?
Pulsus paradoxus is seen in all except?
A young patient presents with a systolic murmur at the apex. The murmur increases with both handgrip and Valsalva maneuver. Which of the following conditions is most likely?
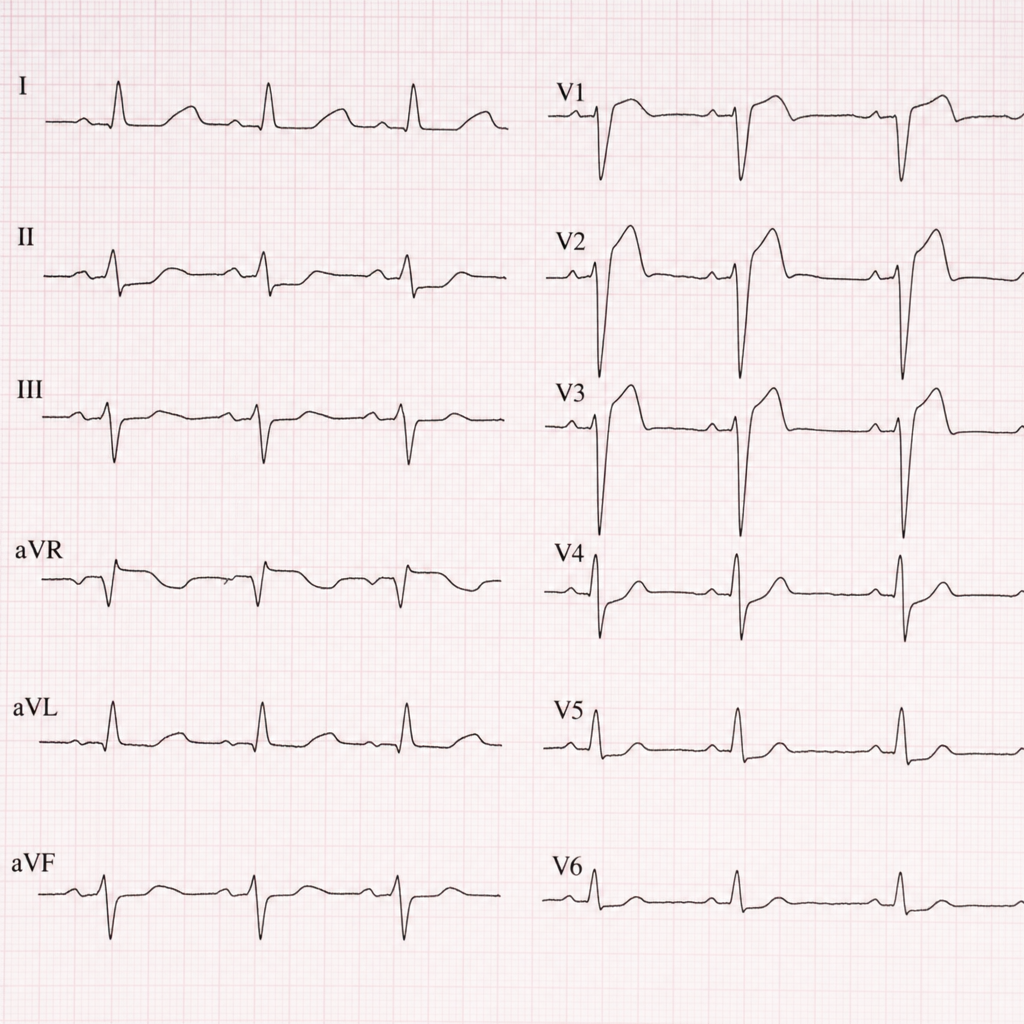
A 38-year-old man develops severe retrosternal chest pain radiating to the back, aggravated by breathing and movement. He has no significant past medical history but had a mild upper respiratory tract infection 1 week ago. His electrocardiogram is shown in Figure. Which of the following is the most likely cause for his condition?
Pulsus paradoxus is characteristically seen in cardiac tamponade. Absence of pulsus paradoxus is seen when cardiac tamponade is associated with all except one of the following?
A 57-year-old man presents with sudden onset of severe and central chest pain radiating to the back. ECG shows ST segment elevation in leads V1-V6, I, aVL. The chest X-ray shows a widened mediastinum. What is the most likely diagnosis?
A 65-year-old hypertensive male presented to the ER with sudden onset of severe, tearing pain in the back of the chest, more so in the interscapular region. He also experienced dyspnea, hemiplegia, hemianesthesia, and frequent episodes of syncope in the past 2 days. On examination, the patient was hypotensive with feeble pulses in bilateral radial arteries, a wide pulse pressure, and a diastolic murmur radiating towards the right sternal border. All of the following are true about the condition except:
A 64-year-old male with a history of anterior Q wave myocardial infarction 4 years ago presents for a routine annual medical checkup. An X-ray reveals findings suggestive of a specific cardiac condition. What is the most likely diagnosis?

All of the following are true for mitral valve prolapse, except?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app