
Cardiology — MCQs

On this page
Which of the following increases the susceptibility to coronary artery disease?
Which one of the following statements is true regarding Stokes-Adams attack?
Prominent x descent in JVP is seen in all EXCEPT?
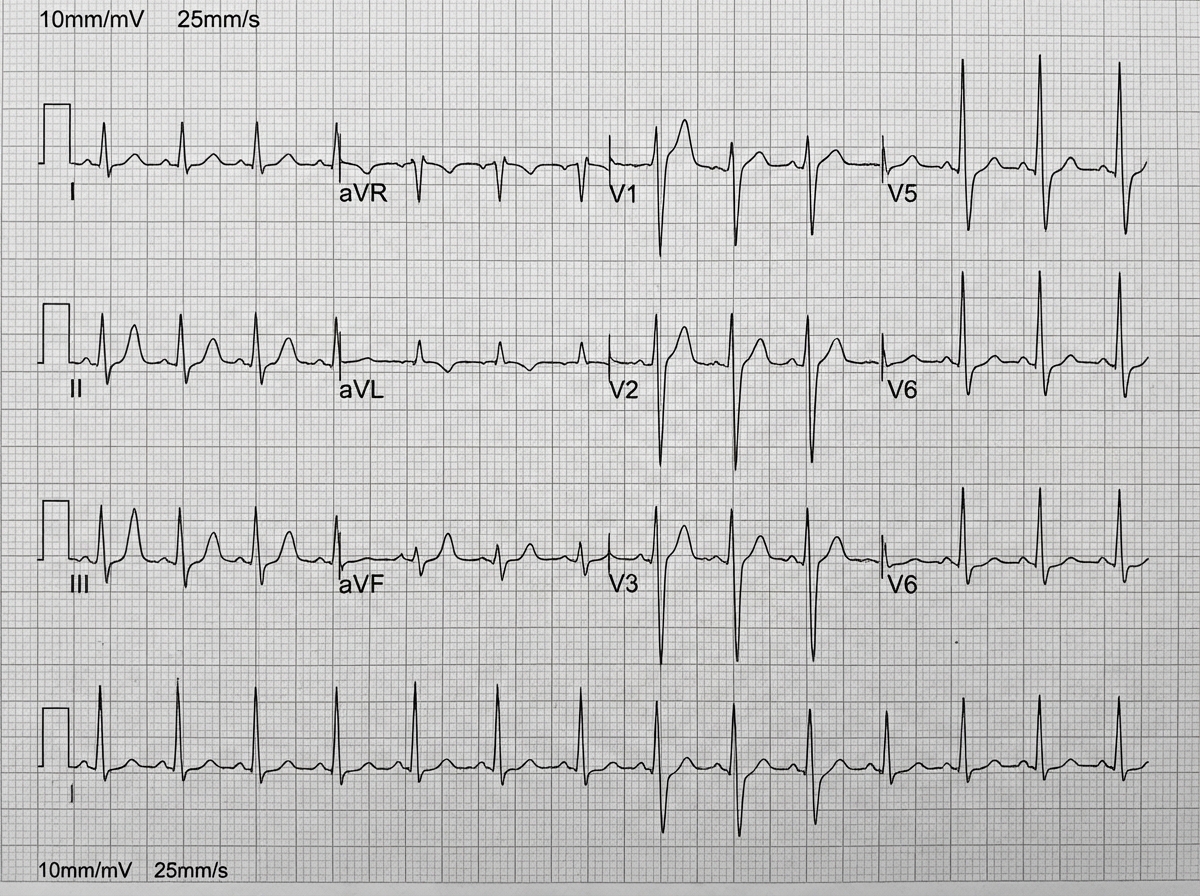
A 50-year-old man presents to the emergency department with chest pain and shortness of breath. He smokes 2 packs of cigarettes daily. His BP is 150/90 mmHg and HR is 110 bpm. An ECG is performed. What is your diagnosis?
Which of the following statements is NOT true regarding myocardial ischemia?
Postural hypotension can be a consequence of which of the following?
Kussmaul's sign is seen in all of the following except?
Where is pulsatile liver and ascites found?
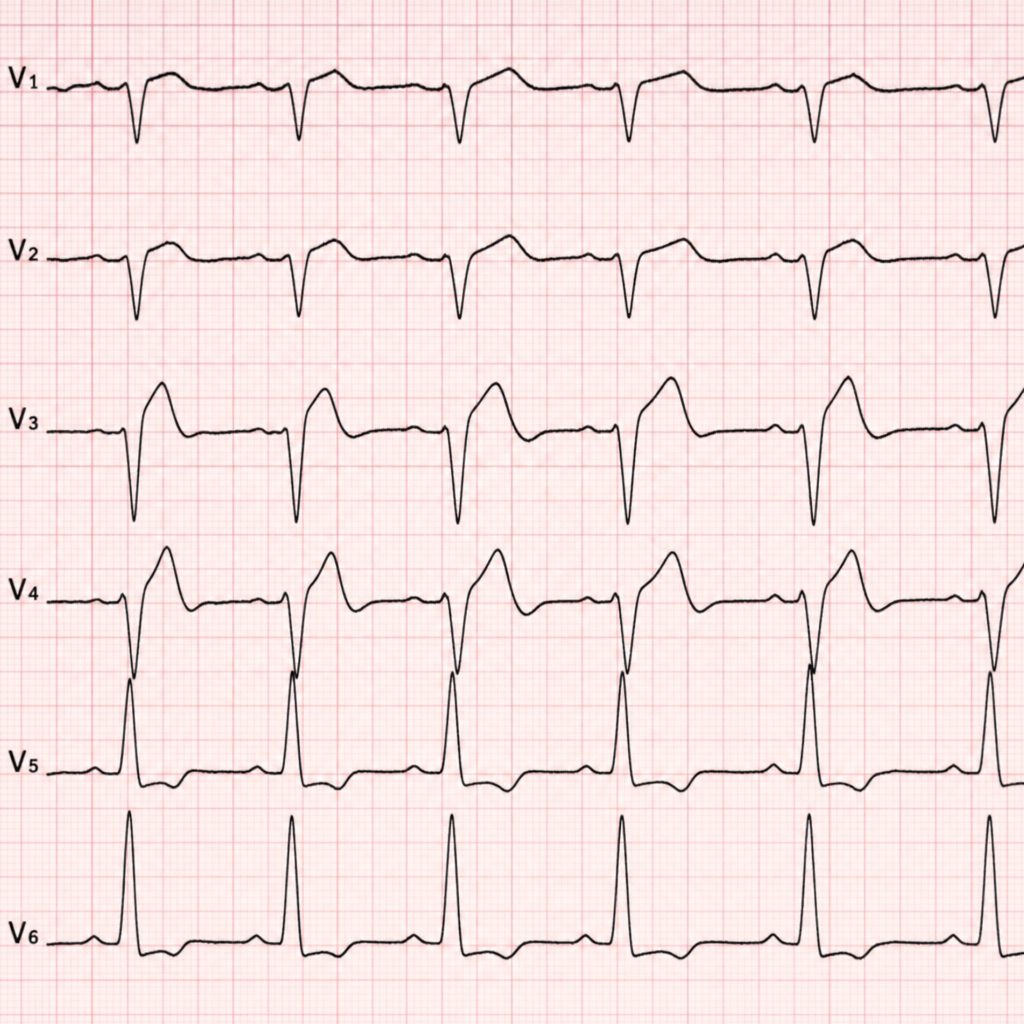
What ECG finding is shown?
Aortic dissection is associated with which of the following?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app