
Cardiology — MCQs

On this page
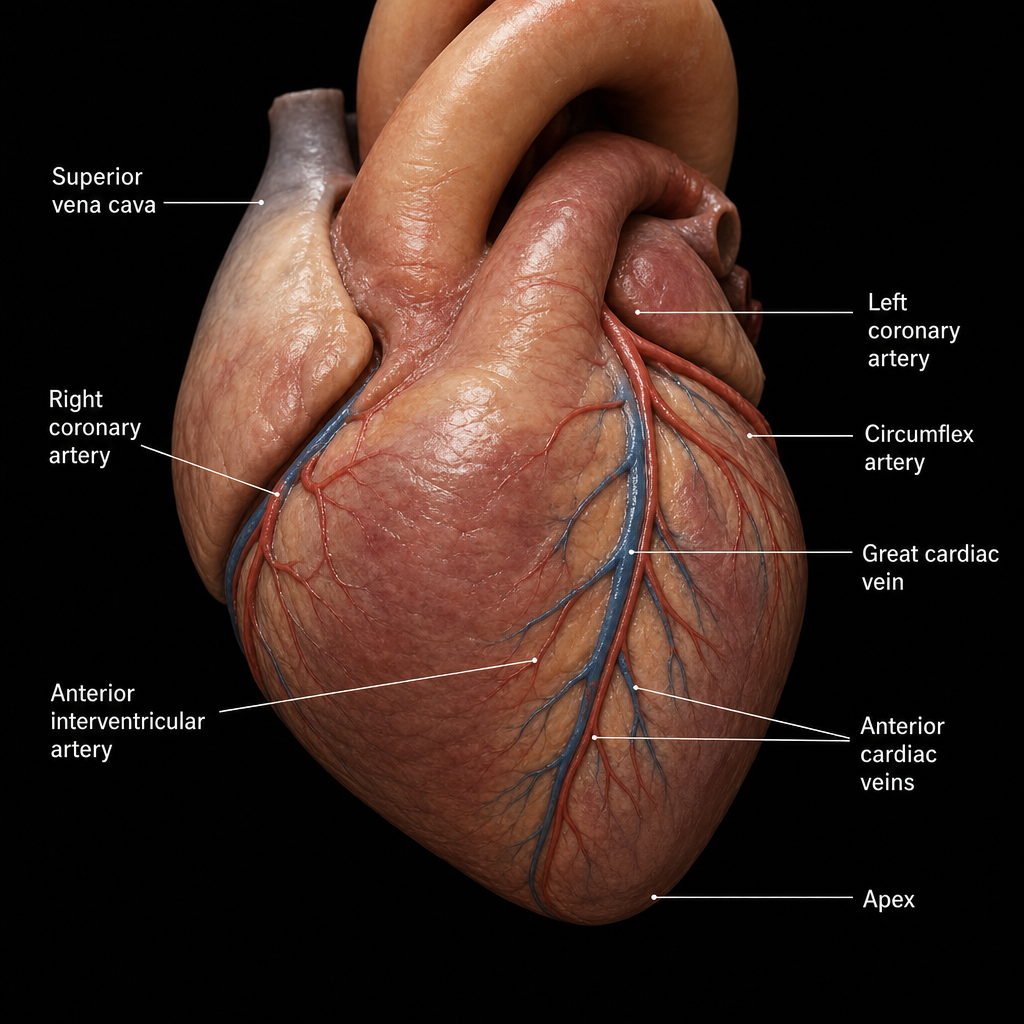
A 50-year-old male presented to the ER with new onset chest pain that was progressively increasing in nature and described as pressure-like chest pain, persisting for more than 20 minutes. ECG showed ST-segment elevation in the anterior leads, and the patient was immediately put on thrombolysis therapy. Which vein is accompanied by the artery involved in this case?
In severe aortic stenosis, which of the following is a true finding?
Which drug is used in unstable angina to prevent myocardial infarction?
J waves (Osborn waves) on ECG are seen in all of the following conditions EXCEPT:
A patient with a moderate ventricular septal defect (VSD) in chronic congestive cardiac failure (CCF) develops clubbing without cyanosis. What is the most likely diagnosis?
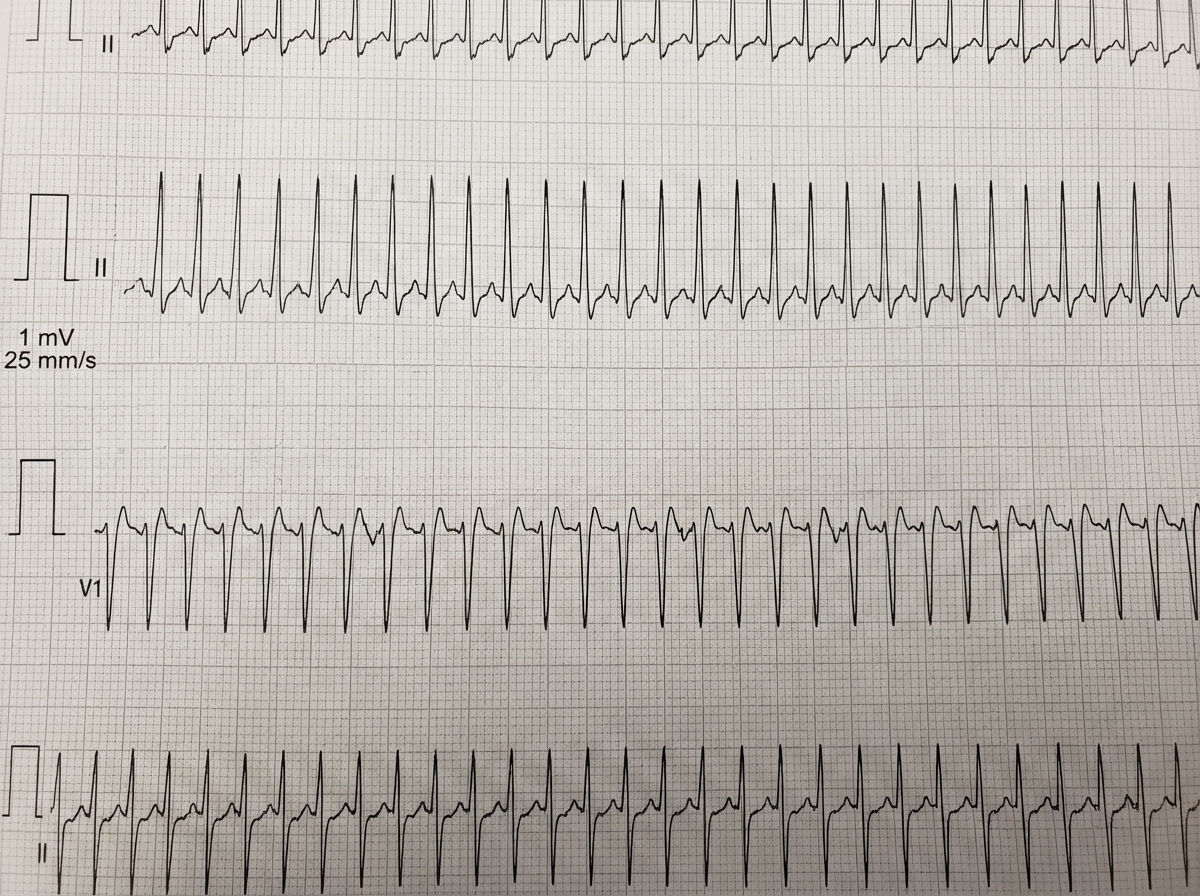
A 36-year-old female presents with a sensation of fast heart rate, slight dizziness, and vague chest fullness. Blood pressure is 110/70. The following rhythm strip is obtained, which shows?
A patient presents 12 hours following a Myocardial infarction. What is the test of choice?
A 37-year-old woman presents with shortness of breath on exertion. She has a past history of rheumatic fever as a child. On cardiac auscultation, there is a loud S1 and a mid-to-late low-pitched diastolic murmur. Which of the following findings is most likely to be seen on the chest X-ray in someone with mitral stenosis?
A 62-year-old man with carcinoma of the lung presented to the emergency department with respiratory distress. His ECG showed electrical alternans. What is the most likely diagnosis?
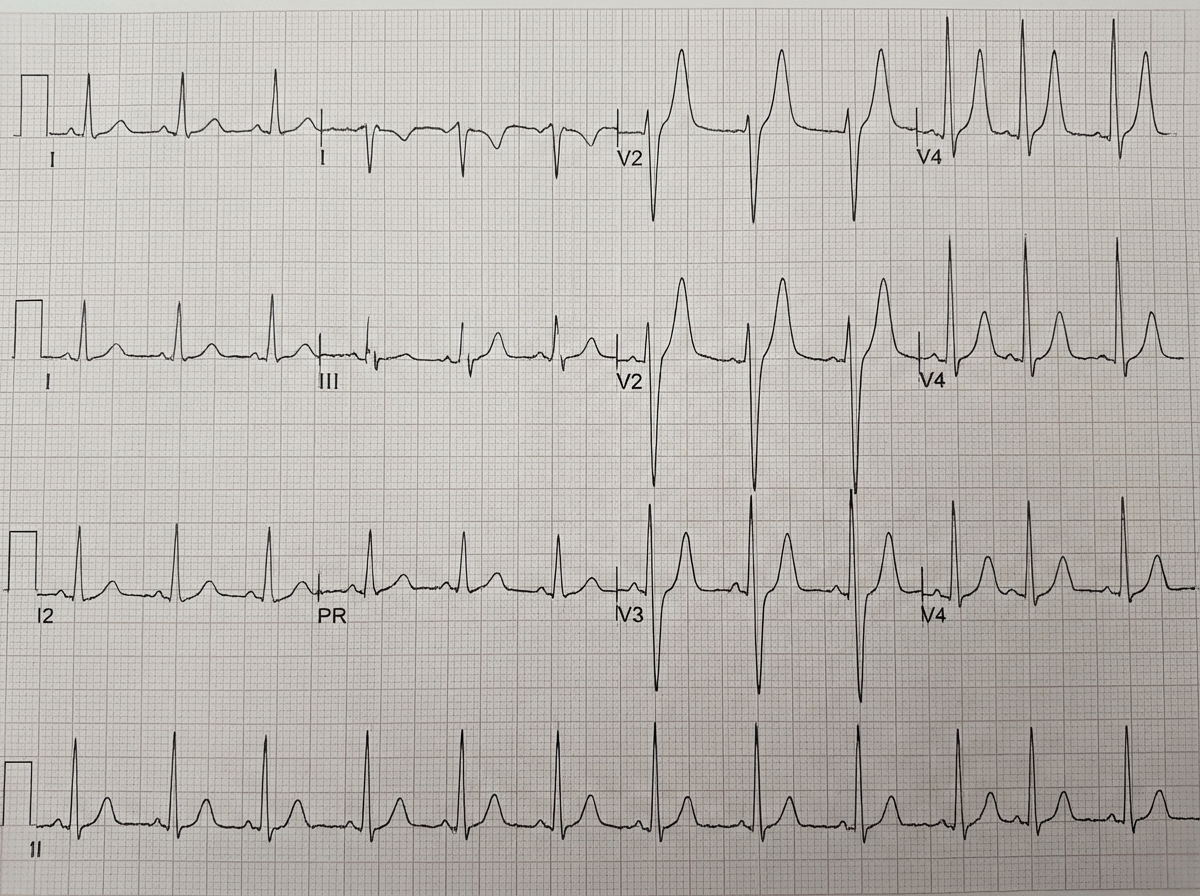
Which electrolyte imbalance is shown in the following ECG?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app