
Cardiology — MCQs

On this page
Reperfusion is useful for which of the following types of myocardium?
All of the following are true about Atrial Septal Defect (ASD) except?
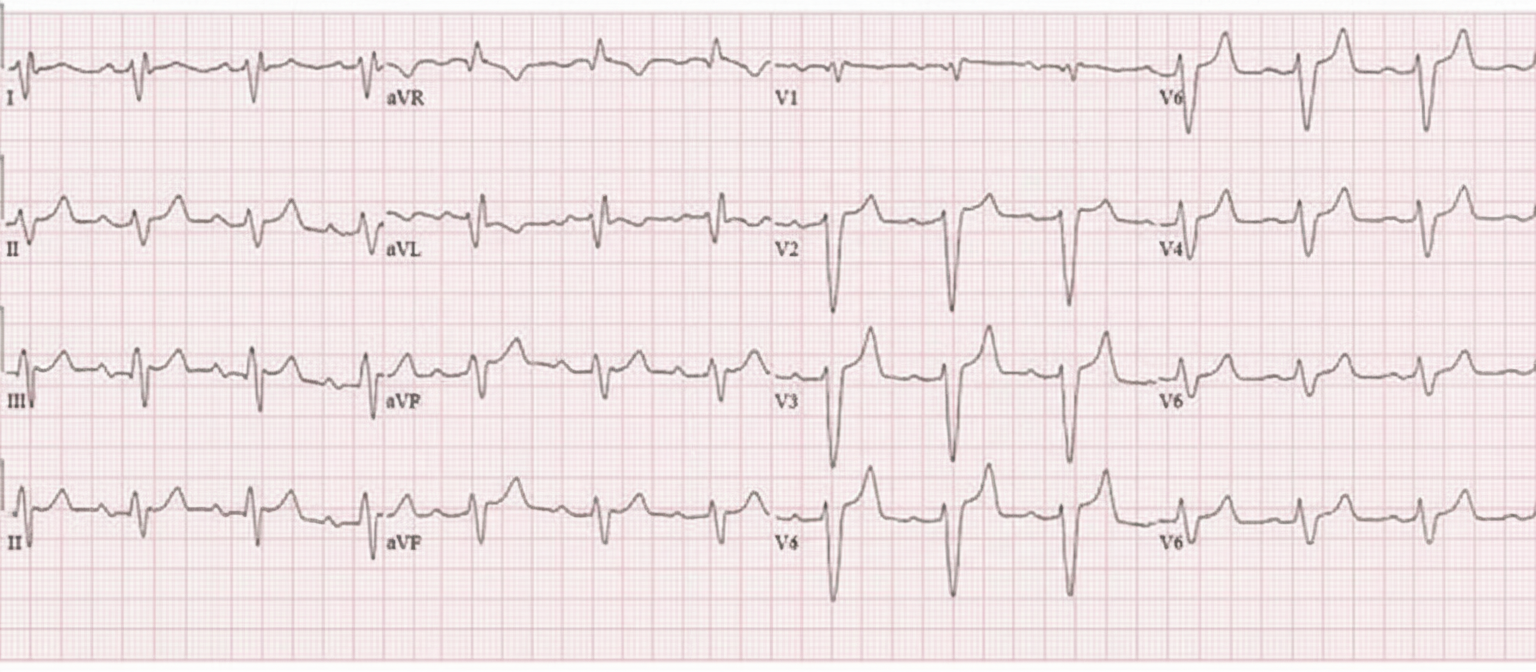
A 50-year-old female patient on losartan and spironolactone therapy for hypertension developed hypotension and bradycardia. Labs show serum potassium 7.2 mEq/L, creatinine 2.8 mg/dL, and arterial blood gas revealing metabolic acidosis (pH 7.21, HCO3 14 mEq/L). The ECG taken is as shown. What is the effective treatment for her condition?
Which of the following is NOT true about Hypertrophic Obstructive Cardiomyopathy?
Which of the following drugs should not be used empirically in the management of isolated systolic hypertension in the elderly?
The most common cause of tricuspid regurgitation is secondary to:
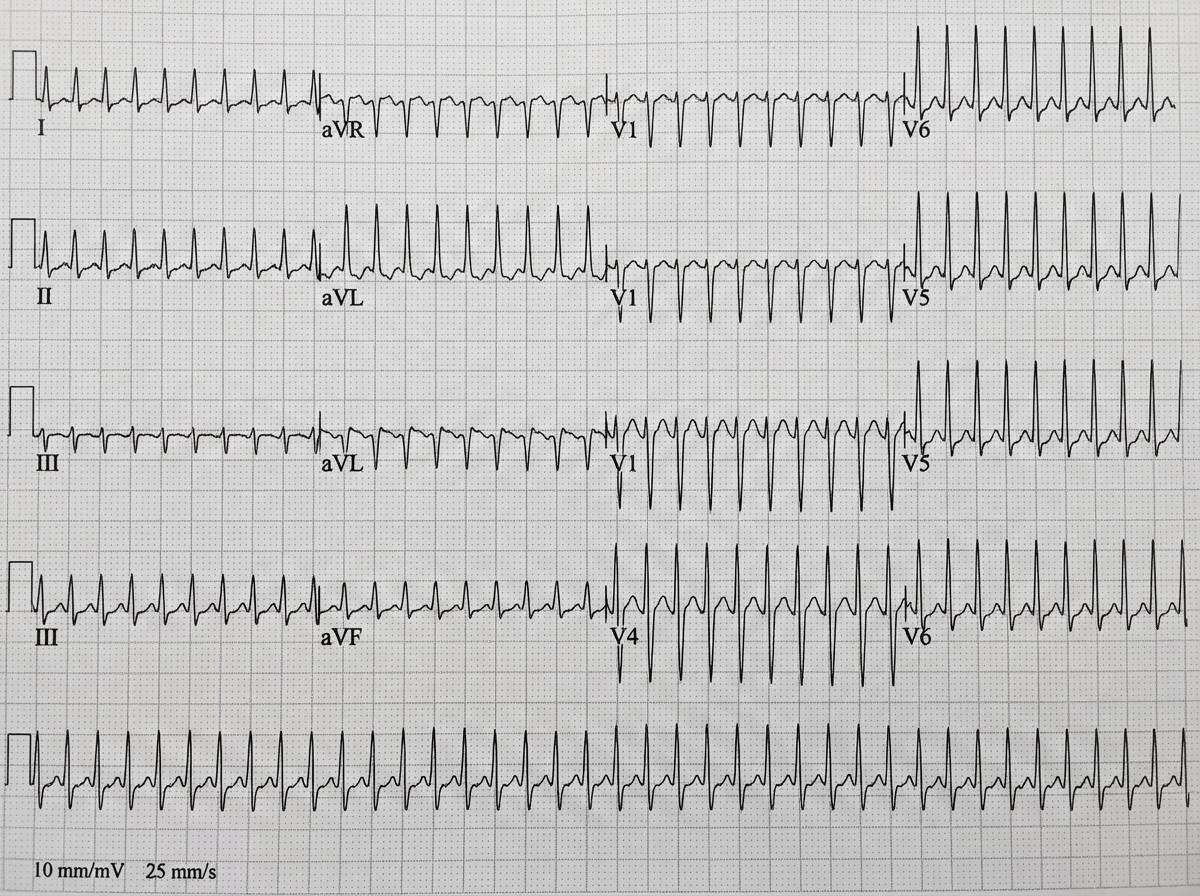
A 36-year-old man presents with the sensation of a racing heart. His blood pressure is 110/70, respiratory rate 14/min, and O2 saturation 98%. ECG is shown. Carotid massage and Valsalva maneuver do not improve the heart rate. Which of the following is the initial therapy of choice?
A 68-year-old male admitted to the ICU for acute exacerbation of COPD develops sudden onset of palpitations. The ECG shows irregular rhythm with varying P wave morphology and varying PR intervals. What is the most likely diagnosis?
A 16-year-old girl presents with chest pain and respiratory distress. On physical examination, she is short of breath, wheezing, and gasping for air. Cardiac auscultation reveals a prominent pansystolic murmur and a prominent third heart sound. Chest X-ray shows marked enlargement of the heart. The patient expired despite intensive supportive measures. Microscopic examination of the myocardium at autopsy discloses aggregates of mononuclear cells arranged around centrally located deposits of eosinophilic collagen. What is the appropriate diagnosis?
Which of the following statements regarding a patient with atrial fibrillation is false?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app