
Cardiology — MCQs

On this page
A 25-year-old patient with a history of recent respiratory tract infection complains of severe chest pain at rest. The ECG of the patient is given. What is the most probable diagnosis?
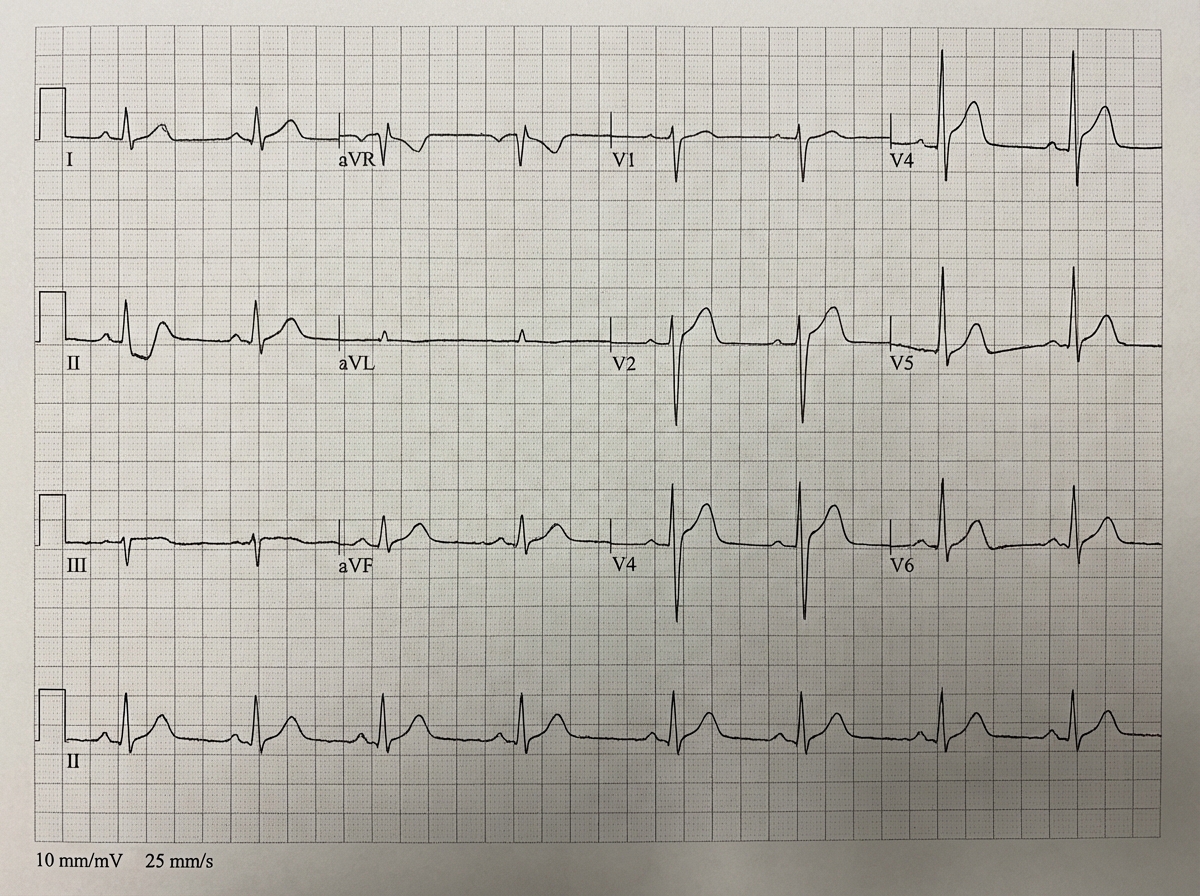
A young man reports retrosternal chest pain over the last few hours. The pain is not related to exertion and is relieved significantly on sitting up and leaning forward. What is the likely diagnosis?
A patient presents with severe chest pain and low-grade fever. The ECG is shown below. What is the most probable diagnosis?
What is the drug of choice in patients with Wolff-Parkinson-White syndrome experiencing atrial fibrillation?
Which of the following statements regarding atrial fibrillation is false?
A 38-year-old woman presented with shortness of breath and fatigue. Her history is unremarkable except for a vague history of fever and joint pain as a child. She notes some recent fatigue and difficulty in sleeping that she attributes to job-related stress. On examination, her heart rate is 120 beats/min. Echocardiogram revealed the following finding. Auscultation of the heart indicates a harsh systolic murmur during left ventricular ejection. Which of the following is NOT a direct consequence of aortic stenosis itself?

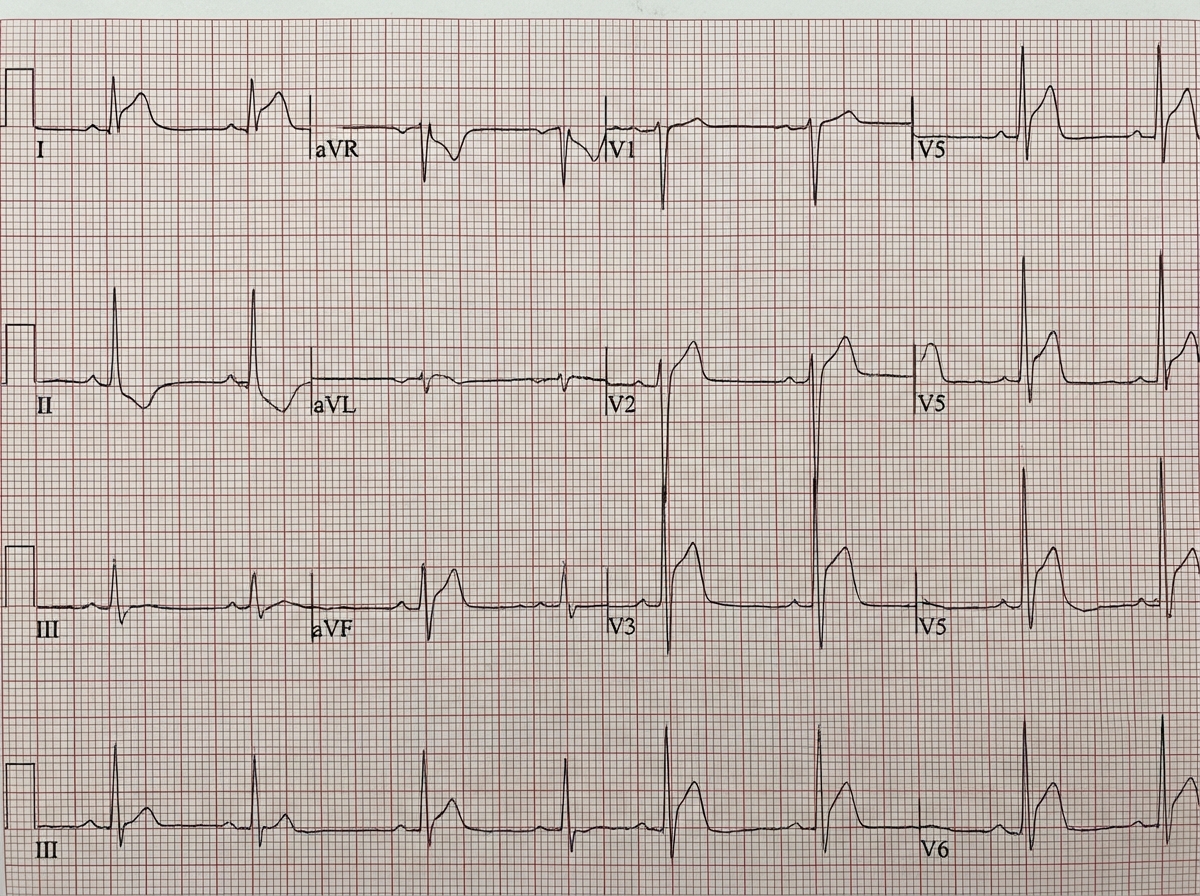
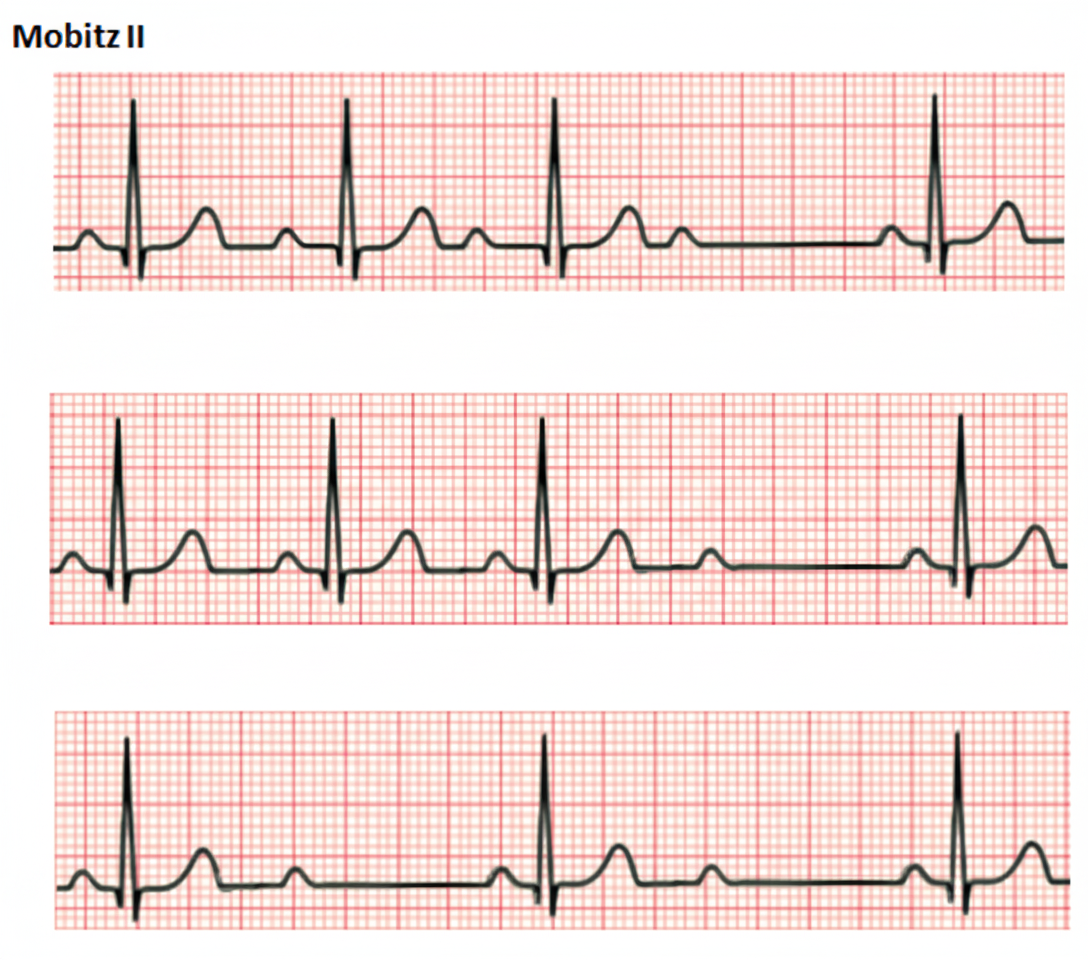
Comment on the diagnosis of the ECG tracing shown below?
A previously healthy 58-year-old man is admitted to the hospital because of an acute inferior myocardial infarction. Within several hours, he becomes oliguric and hypotensive (blood pressure is 90/60 mmHg). Insertion of a pulmonary artery (Swan-Ganz) catheter reveals the following pressures: pulmonary capillary wedge pressure - 4 mmHg; pulmonary artery pressure - 22/4 mmHg; and mean right atrial pressure - 11 mmHg. How would this patient be best treated?
Which of the following are predisposing factors for Coronary Artery Disease?
A 20-year-old patient presents with syncope. His ECG shows specific findings, and his elder brother died suddenly. A subsequent cardiac MRI revealed fibro-fatty changes in the RV myocardium. What is the most likely diagnosis for this patient?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app