
Cardiology — MCQs

On this page
Unequal pulses in upper and lower extremities (i.e., radio-femoral delay) is/are seen in which of the following conditions?
A 70-year-old male patient presented to the emergency department with pain in the epigastrium and difficulty in breathing for 6 hours. On examination, his heart rate was 56 beats per minute and the blood pressure was 106/60 mm Hg. Chest examination was normal. The patient has been taking omeprazole for gastroesophageal reflux disease for the last 6 months. What should be the initial investigation?
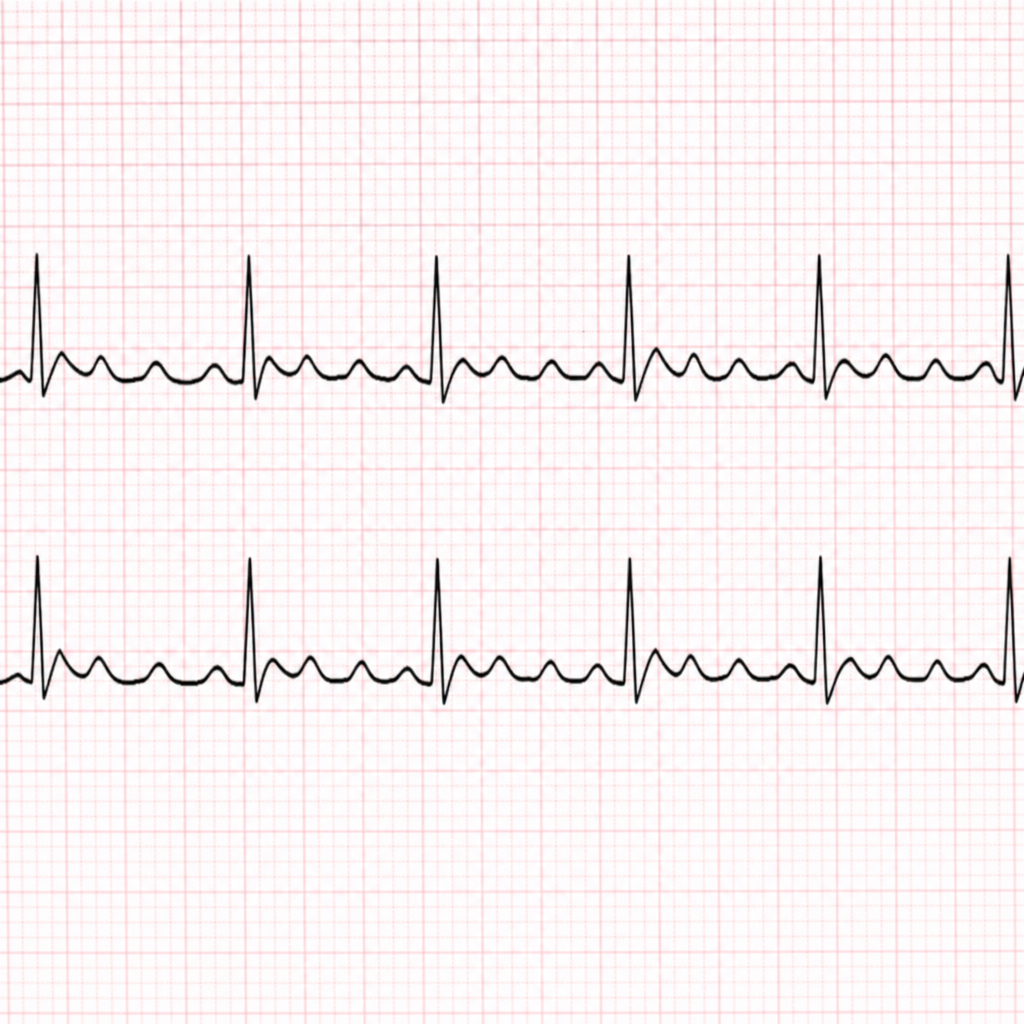
A 62-year-old man with underlying COPD develops a viral upper respiratory infection and begins taking an over-the-counter decongestant. Shortly thereafter he experiences palpitations and presents to the emergency room, where the following rhythm strip is obtained. What is the most likely diagnosis?
Which one of the following findings is NOT associated with left-sided heart failure?
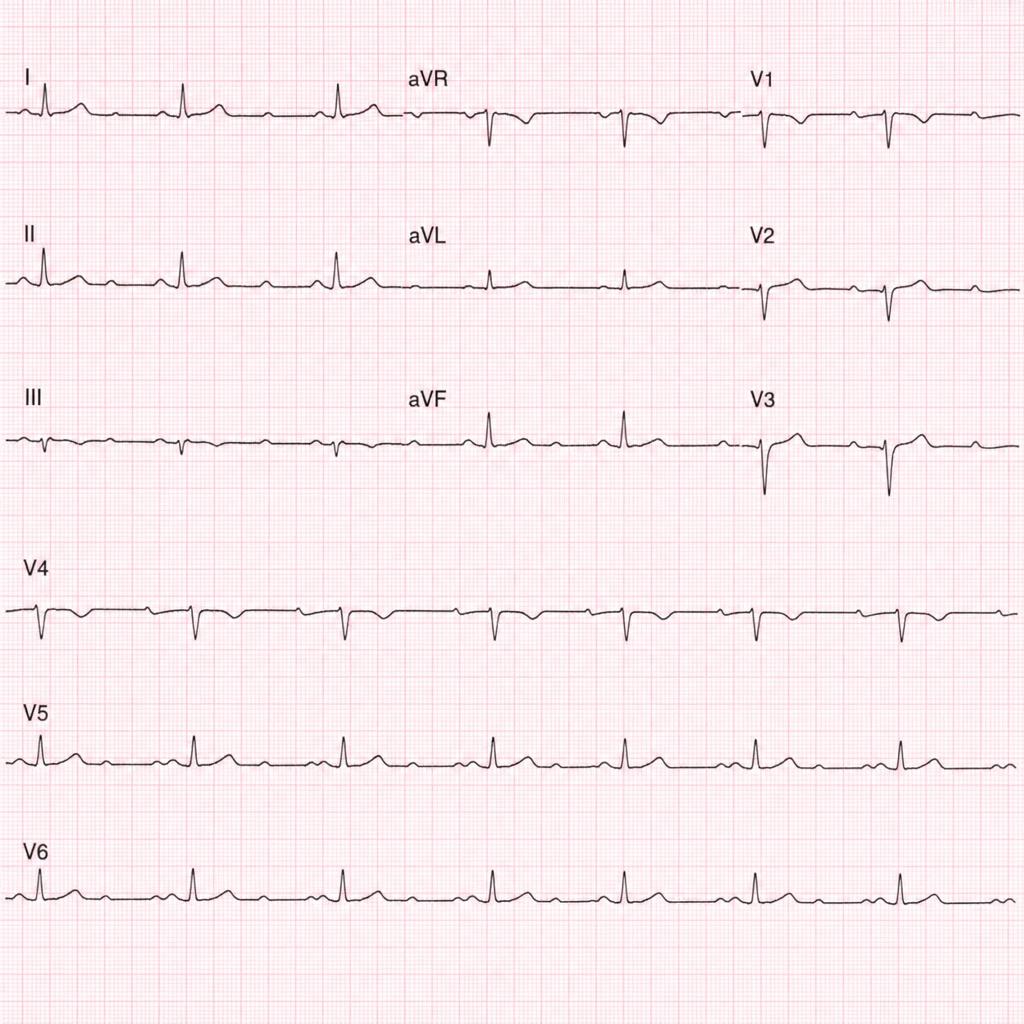
A 30-year-old man presents with recurrent attacks of feeling dizzy. An ECG was performed. What is the most likely diagnosis?
What is the most common cause of sudden cardiac death?
The Bundle of Kent is associated with which of the following conditions?
Giant a waves in JVP are seen in which of the following conditions?
Bacterial endocarditis is rarely seen in which of the following cardiac conditions?
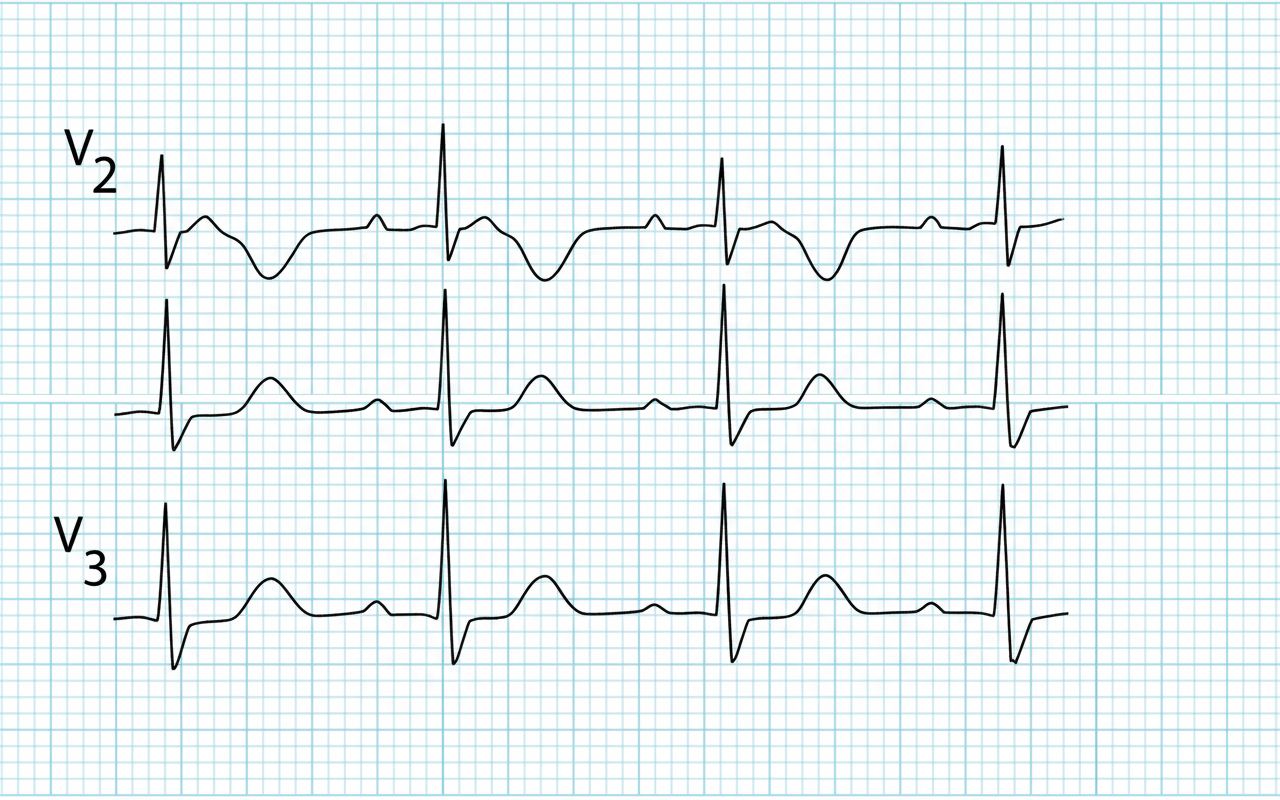
Comment on the ECG finding shown below?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app