
Cardiology — MCQs

On this page
In a patient with wide-complex tachycardia, the presence of all of the following in the ECG indicates ventricular tachycardia except?
A study of risk factors for atherogenesis in adults is performed. Which of the following substances is most likely to reduce serum cholesterol?
A 32-year-old man involved in a high-speed road traffic accident is found unconscious at the scene and breathing spontaneously. In the emergency department, the ECG monitor shows an irregular rhythm with no discernible P waves, QRS complexes, ST segments, or T waves, and a rapid rate. What is the best management for this patient?
Pericardial knock is heard in which condition?
A 70-year-old man with a history of coronary artery disease presents with substernal chest pressure, diaphoresis, and nausea, along with difficulty catching his breath. An electrocardiogram shows septal T-wave inversion. His troponin I is elevated. He has been given aspirin and sublingual nitroglycerin. Blood pressure is 154/78 and heart rate is 72. What is the best next step in management?
A 75-year-old woman with hypertension develops fatigue and dyspnea on exertion. Her blood pressure is 160/60 mm Hg and pulse 80/min. The second heart sound is diminished and there is an early diastolic murmur that radiates from the right sternal border to the apex. Your clinical diagnosis is aortic regurgitation. What is the characteristic arterial pulse finding for this patient?
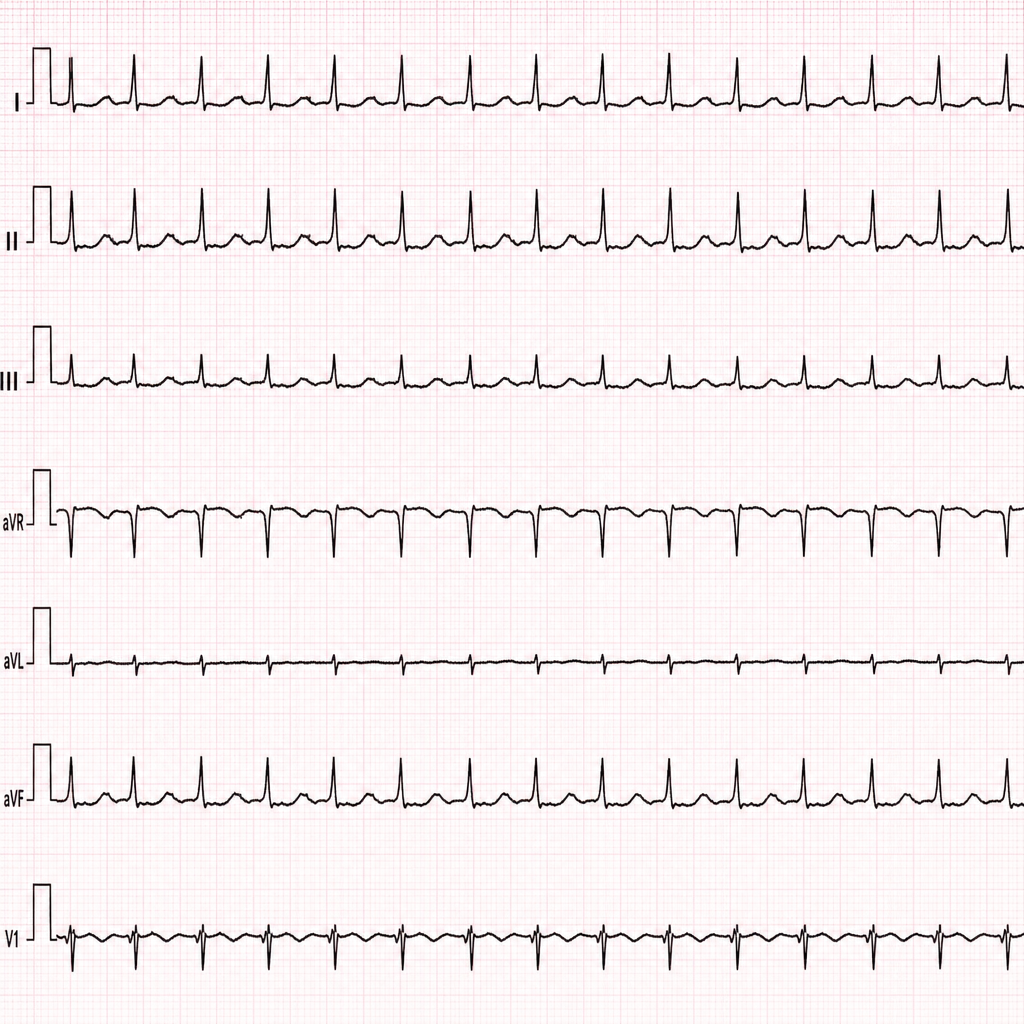
A 36-year-old white female nurse comes to the ER due to a sensation of fast heart rate, slight dizziness, and vague chest fullness. Blood pressure is 110/70. The following rhythm strip is obtained, which shows?
QT prolongation is seen in all, EXCEPT?
All of the following are true about Right Ventricular Infarcts, except?
Which of the following results in broad complex tachycardia?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app