
Cardiology — MCQs

On this page
All of the following statements are TRUE about infectious endocarditis EXCEPT?
What TIMI score on angiography denotes complete occlusion of a coronary artery?
A 42-year-old man with known valvular heart disease develops a fever for 1 week. He appears unwell; findings include a pansystolic murmur at the apex that radiates to the axilla and a soft S1 sound. He has petechiae on his conjunctival sac, linear hemorrhages under a few fingernails, and painful, tender, and erythematous nodules on some of the distal fingertips. Which of the following is the most responsible mechanism for these physical findings?
Which of the following auscultatory signs is absent in mitral stenosis when atrial fibrillation is present?
Which of the following is NOT an X-ray feature of Atrial Septal Defect?
Which of the following statements regarding peripartum cardiomyopathy is true?
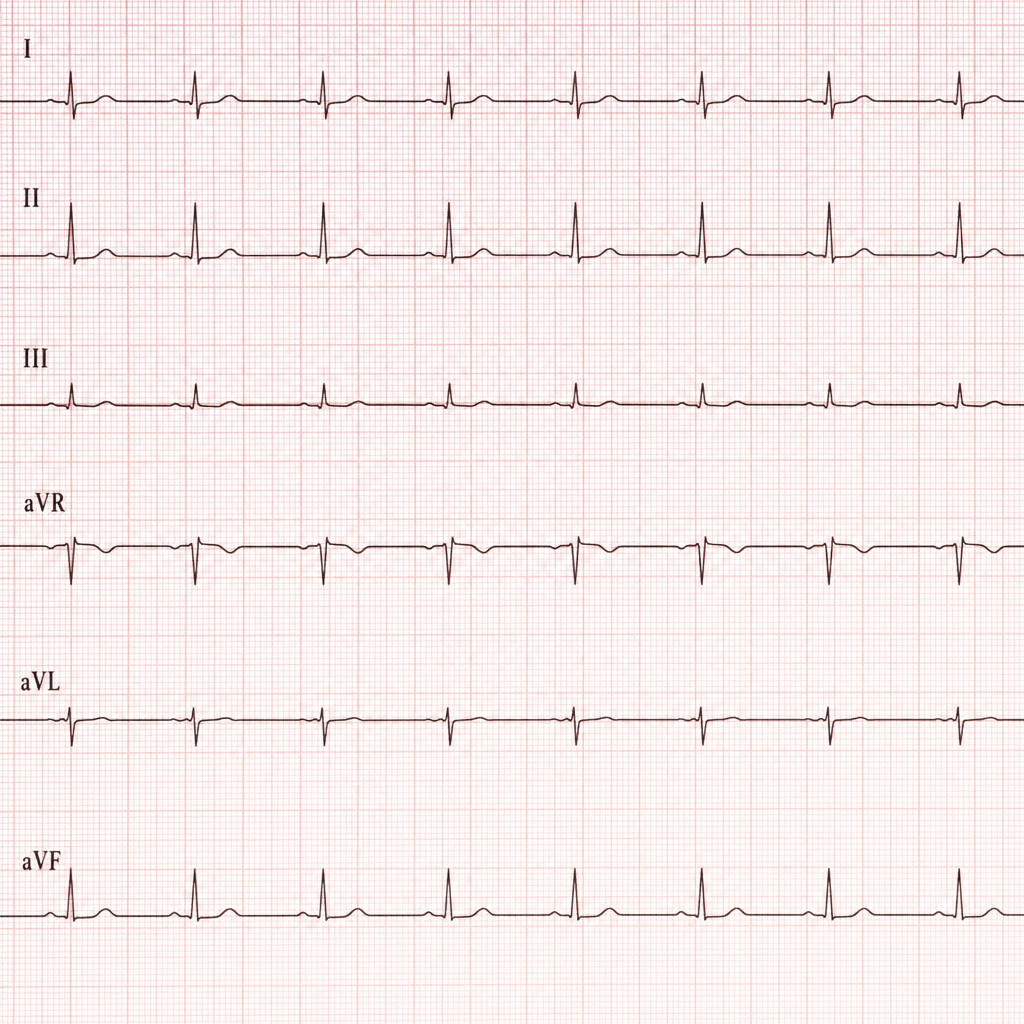
Which of the following describes the marked ECG finding?
A previously healthy 65-year-old woman presents with acute stroke. Examination reveals acute bilateral lower extremity deep vein thrombosis. Echocardiogram with agitated saline contrast shows bubbles crossing into the left atrium. Which of the following is most likely responsible for her symptoms?
A 58-year-old man presents with chest pain that occurs on exertion and resolves with rest. The pain is not present at rest and always remits spontaneously within a few minutes. His blood pressure is mildly elevated at 145/85 mmHg, and his ECG shows normal sinus rhythm. What is the most appropriate investigation?
Which of the following is a major criterion for the diagnosis of Rheumatic fever according to the modified Jones criteria?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app