
Cardiology — MCQs

On this page
A patient presents with sharp, shooting retrosternal pain that progresses downward, initially felt between the scapulae and later migrating to the epigastric region. On examination, the patient has feeble lower limb pulses compared to the upper limbs. This clinical presentation is highly suggestive of which of the following conditions?
Which of the following is a contraindication to chemical cardioversion?
Gorlin's formula is used to calculate what parameter?
A patient had an inferior wall myocardial infarction and was in shock. What is the most likely reason for the patient being in shock?
All of the following ECG features indicate ventricular tachycardia except?
A young female presents with a history of dyspnea on exertion. On examination, she has wide, fixed split S2 with an ejection systolic murmur in the left second intercostal space. Her EKG shows left atrial deviation. What is the most probable diagnosis?
The ECG of a patient with an artificial pacemaker in the right ventricle shows?
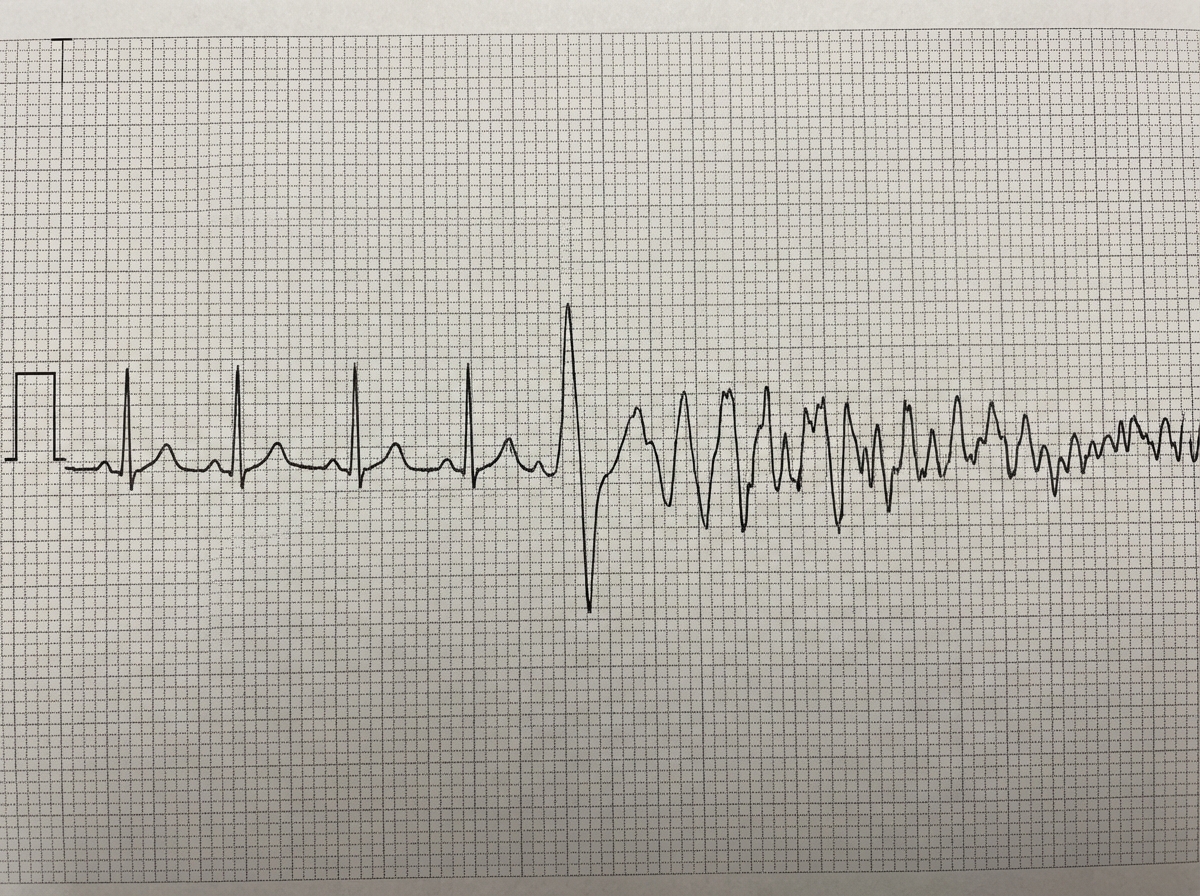
A 50-year-old man presents with central chest pain. He collapsed while his ECG was being recorded. What is the cause of this ECG?
Atrial fibrillation is seen in all of the following conditions EXCEPT:
A 50-year-old man has been experiencing fainting episodes for approximately 2 weeks. During these episodes, his ECG reveals a ventricular rate of 25 beats per minute and a P wave rate of 100 beats per minute. The episodes last about 30 seconds, after which a normal sinus rhythm spontaneously recurs. What is the most likely diagnosis?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app