
Cardiology — MCQs

On this page
All statements are true regarding non-ST elevation acute coronary syndromes (NSTE-ACS) and ST elevation myocardial infarctions (STEMI) except?
A 27-year-old woman presents with cough, shortness of breath, and palpitations. Her childhood history includes recurrent "pneumonia." She denies sputum production. On examination, she appears anxious, with distended neck veins, a widened split second heart sound with minimal respiratory variation, and a systolic ejection murmur in the pulmonic area. Lung examination reveals bilateral crackles, mild ascites, and pedal edema. EKG shows right axis deviation. What is the next diagnostic step?
What is the most common congenital cardiac anomaly diagnosed in adulthood?
Spurious hypertension (false elevation of blood pressure readings) is most commonly associated with which of the following findings?
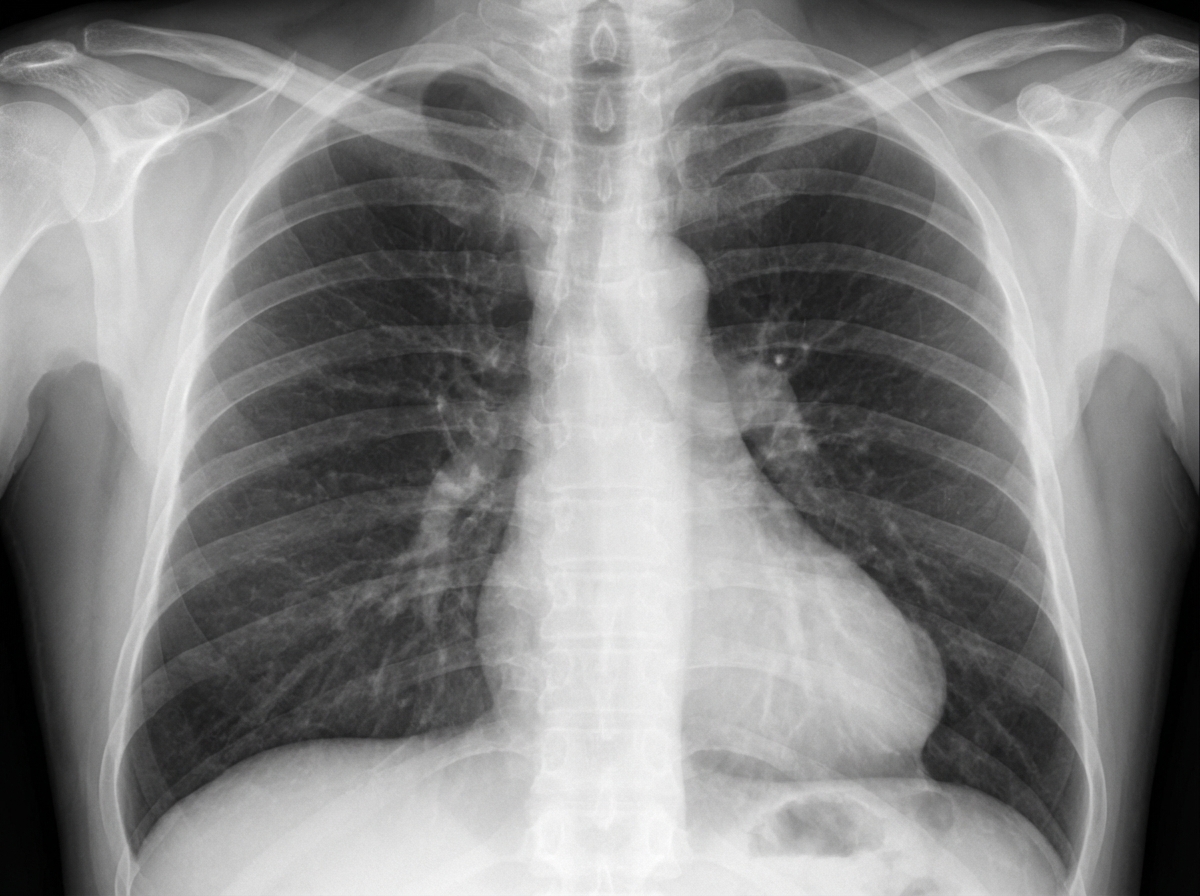
A 67-year-old male smoker presents with cough and was treated for acute bronchitis. A chest X-ray prompted a referral to the chest clinic. The patient has a past history of myocardial infarction but is currently asymptomatic. Blood pressure is 128/80, and cardiopulmonary examination is unremarkable. A purified protein derivative (PPD) test result is 7 mm. The chest X-ray is shown. What is the likely diagnosis?
What is the treatment of choice for hypertension in patients with diabetes mellitus?
A 57-year-old man comes to see you for follow-up 4 weeks after being discharged from hospital for unstable angina. His coronary angiogram showed moderate nonstenotic disease in two vessels. The cardiologist asks you to follow up on his fasting lipid profile since it was not checked in the hospital. His T-chol is 240 mg/dL, LDL 120 mg/dL, HDL 50 mg/dL, and triglycerides 130 mg/dL. For the above patient with dyslipidemia, select the most appropriate treatment?
All of the following statements about pulse deficit in Atrial Fibrillation are true, except?
A young lady complains of sudden onset of palpitations, extreme weakness, and sweating. On examination, she was found to have a blood pressure of 90/70 mmHg with a regular pulse rate of 180/minute. Her symptoms disappeared after vomiting but she complained of polyuria. What is the most likely diagnosis?
JVP wave with absent y descent and prominent x wave is seen in which condition?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app