
Cardiology — MCQs

On this page
A 50-year-old man has a 2-year history of angina pectoris that occurs during exercise. On physical examination, his blood pressure is 135/75 mm Hg, and his heart rate is 79/min and slightly irregular. Coronary angiography shows a fixed 75% narrowing of the anterior descending branch of the left coronary artery. He has several risk factors for atherosclerosis: smoking, hypertension, and hypercholesterolemia. Which of the following is the earliest event resulting from the effects of these factors?
Severity of mitral stenosis is judged by?
A 60-year-old mildly obese woman presents with recurrent chest pain on exertion, which has occurred over several years. She also reports painful leg cramps when walking. Her fasting blood glucose is 160 mg/dL and total serum cholesterol is 370 mg/dL. The ECG is normal and cardiac-specific proteins are negative. What is the most likely underlying condition causing her chest pain?
Destination therapy is indicated in which of the following conditions?
Which of the following is true regarding an opening snap?
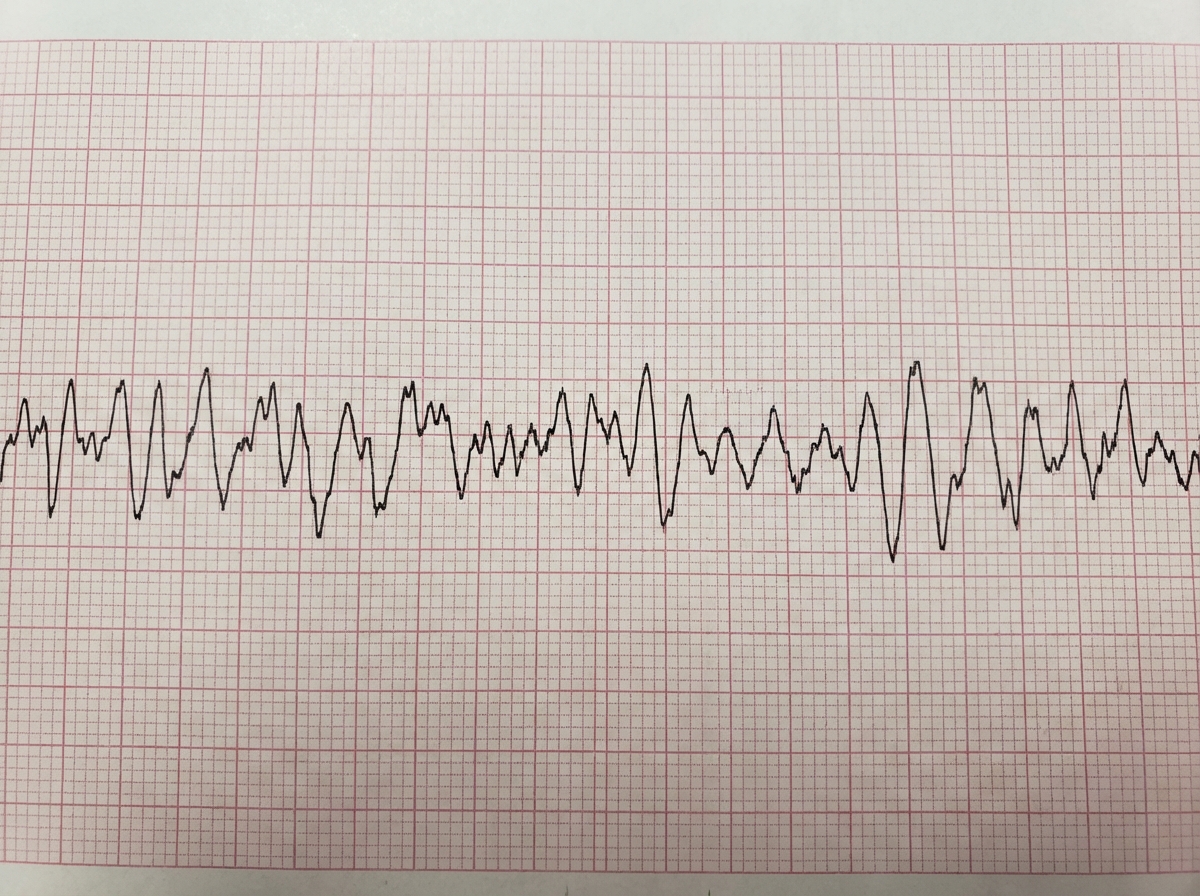
A 65-year-old man, who is on aspirin, statins, and beta-blockers for chronic stable angina, develops chest pain for the past 4 hours. He becomes unconscious and unresponsive while talking to the doctor on duty. He is found to have no pulse, and the immediately available defibrillator displays ventricular fibrillation (VF). An ECG was done. What is the best step for management of this patient?
What is the most common cause of acute cor pulmonale?
What is the characteristic JVP finding in right ventricular infarction?
All of the following conditions are more commonly associated with LBBB pattern than RBBB pattern on ECG, except?
Inferoposterior wall myocardial infarction will show changes in which of the following leads?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app