
Cardiology — MCQs

On this page
Which of the following ECG findings would indicate a posterior wall myocardial infarction?
Which valve is most commonly affected in subacute bacterial endocarditis?
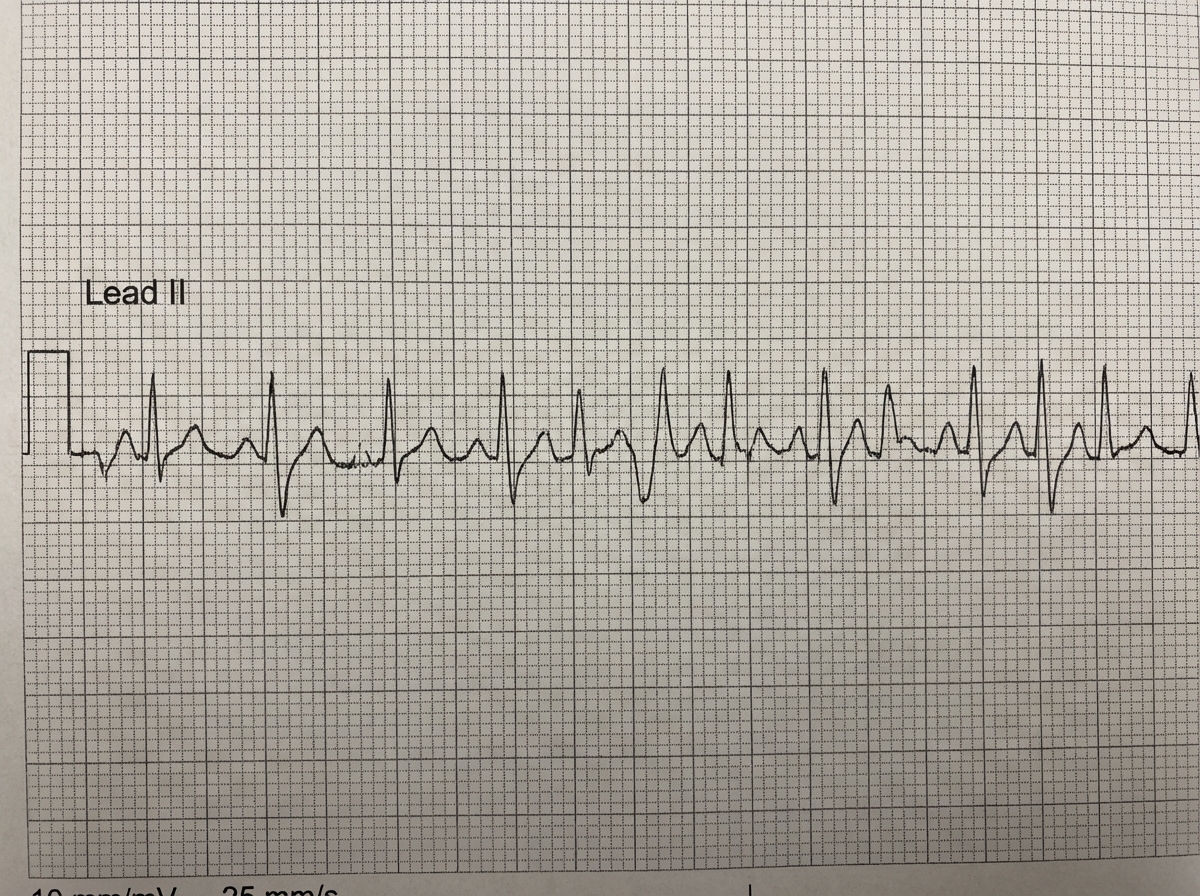
A 62-year-old male with underlying COPD develops a viral upper respiratory infection and begins taking an over-the-counter decongestant. Shortly thereafter, he experiences palpitations and presents to the emergency room, where the given rhythm strip is obtained, demonstrating:
Which of the following conditions presents with an ECG pattern that mimics myocardial infarction, often referred to as 'myocardial stunning'?
The ECG in hyperkalemia classically shows:
Which gene alteration is most commonly associated with dilated cardiomyopathy?
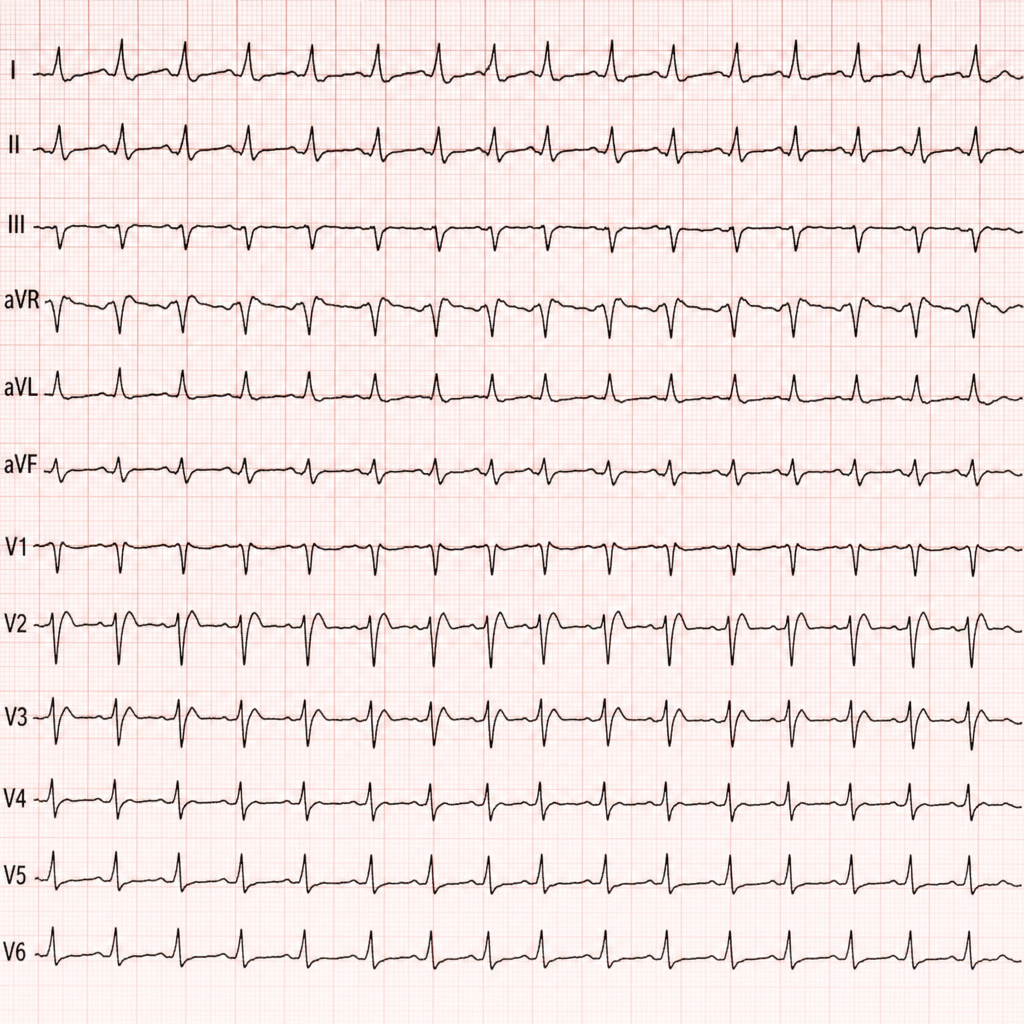
Comment on the diagnosis of the patient based on ECG?
A fixed PR interval with occasional dropped beats in a 2:1, 3:1, or 4:1 pattern, accompanied by a wide QRS complex, is characteristic of which condition?
What is the most common cause of embolism leading to cerebrovascular disease?
A 45-year-old man presents to the emergency department with dizziness. He has a history of supraventricular beats and is currently taking aspirin, atenolol, and quinine. His EKG reveals Torsades De Pointes. How should he be managed?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app