
Cardiology — MCQs

On this page
A 21-year-old male presents with exertional dyspnea, raised JVP, and loud P2. ECG shows right axis deviation. All of the following conditions are possible except?
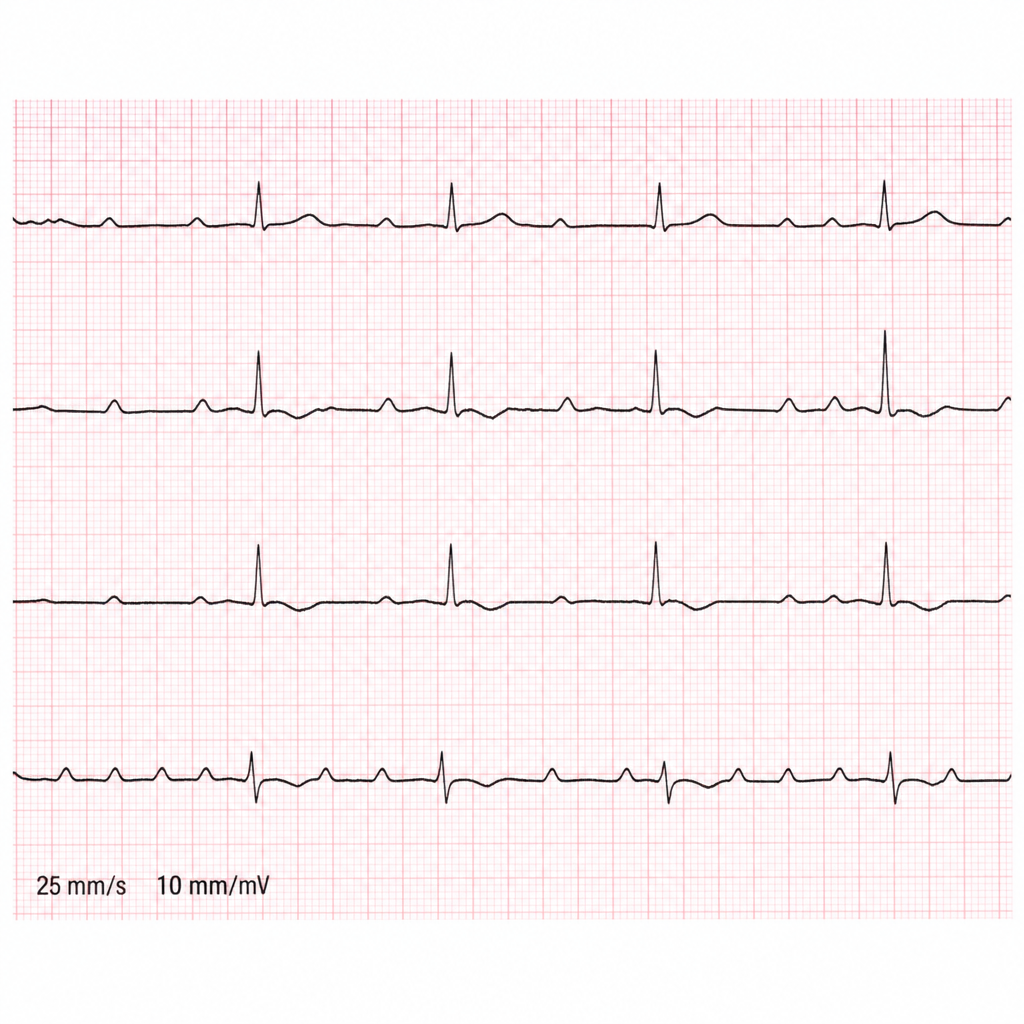
A 62-year-old male with underlying COPD develops a viral upper respiratory infection and begins taking an over-the-counter decongestant. Shortly thereafter he experiences palpitations and presents to the emergency room, where the following rhythm strip is obtained, demonstrating what rhythm?
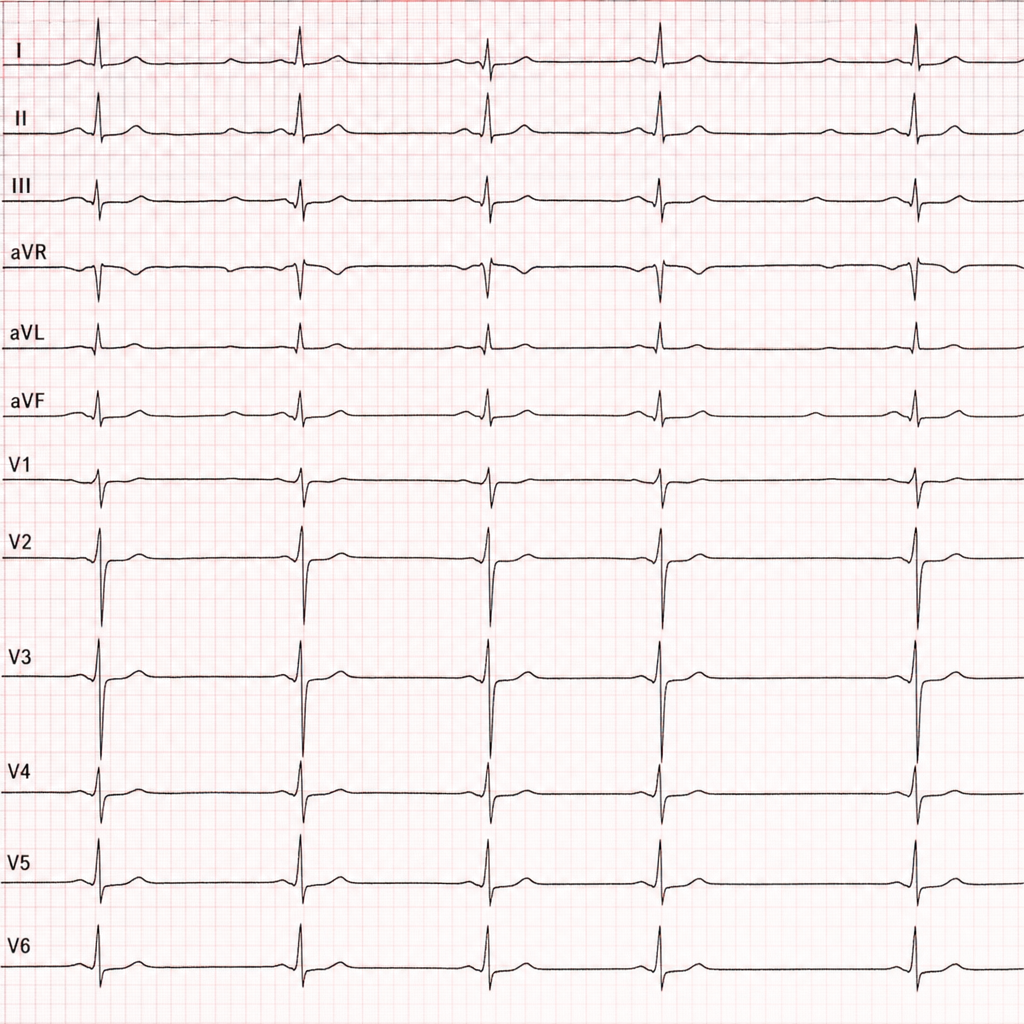
The following ECG shows:
All of the following are considered minor criteria for infective endocarditis EXCEPT?
Quincke's sign in aortic regurgitation refers to which of the following?
The Framingham Risk Score is used to determine which of the following?
A patient with mitral stenosis has developed pulmonary artery hypertension. Which of the following auscultatory findings may be heard?
All of the following features can differentiate between ventricular tachycardia and supraventricular tachycardia EXCEPT?
What is the drug of choice for Paroxysmal Supraventricular Tachycardia?
Which condition is characterized by a reduced PR interval?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app