
Cardiology — MCQs

On this page
Which of the following conditions are typically associated with a continuous murmur?
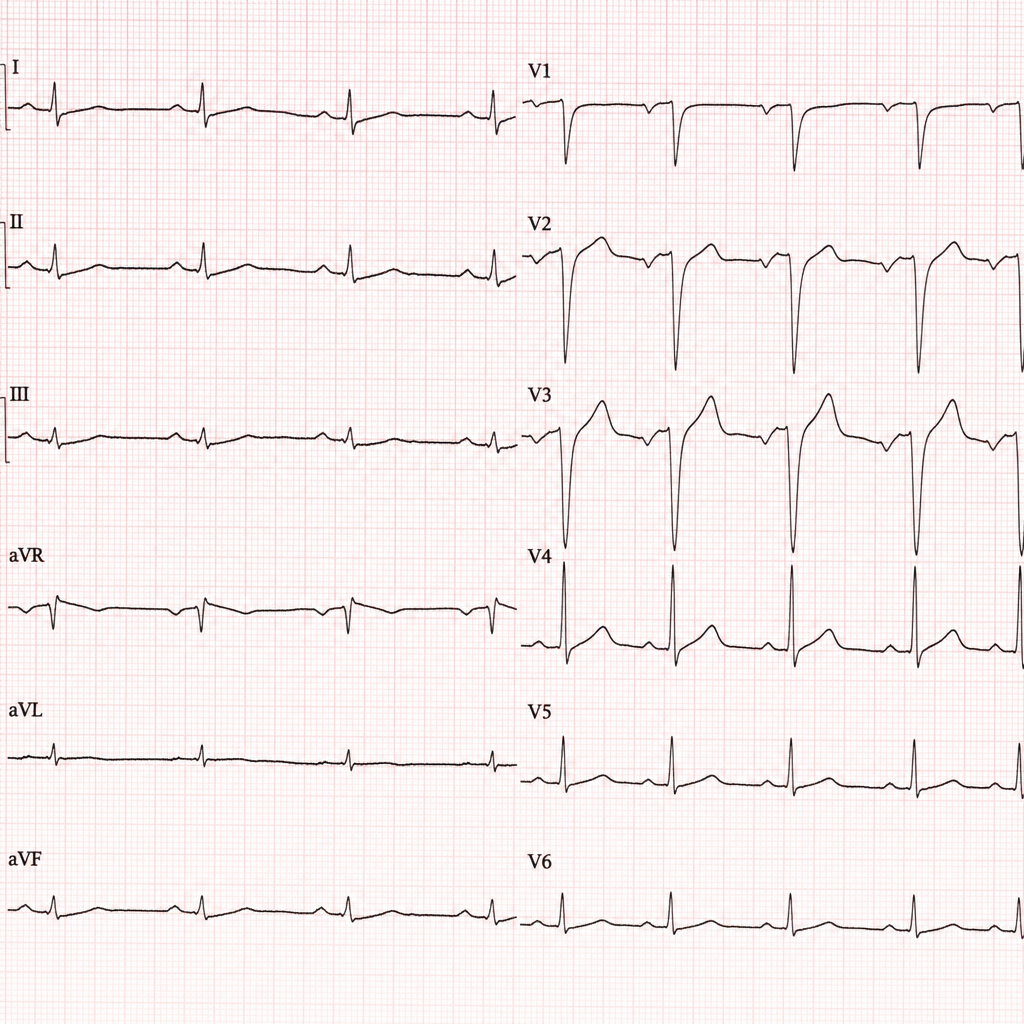
Comment on the diagnosis?
J waves are typically seen in which of the following conditions?
Regarding Wolf-Parkinson-White (WPW) syndrome, which of the following statements is incorrect?
What is considered a wide QRS duration?
A 68-year-old man presents with progressive shortness of breath. He had a metallic heart valve replacement 13 years ago for severe aortic stenosis. Which of the following clinical findings is most indicative of a failing aortic valve replacement?
What is the most common infection in patients with prosthetic valves?
Which of the following is associated with atherosclerosis?
What is the treatment of choice for congestive heart failure with hypertension?
A patient develops sudden palpitation with a heart rate of 150 beats per minute, which is regular. What could be the cause?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app