
Cardiology — MCQs

On this page
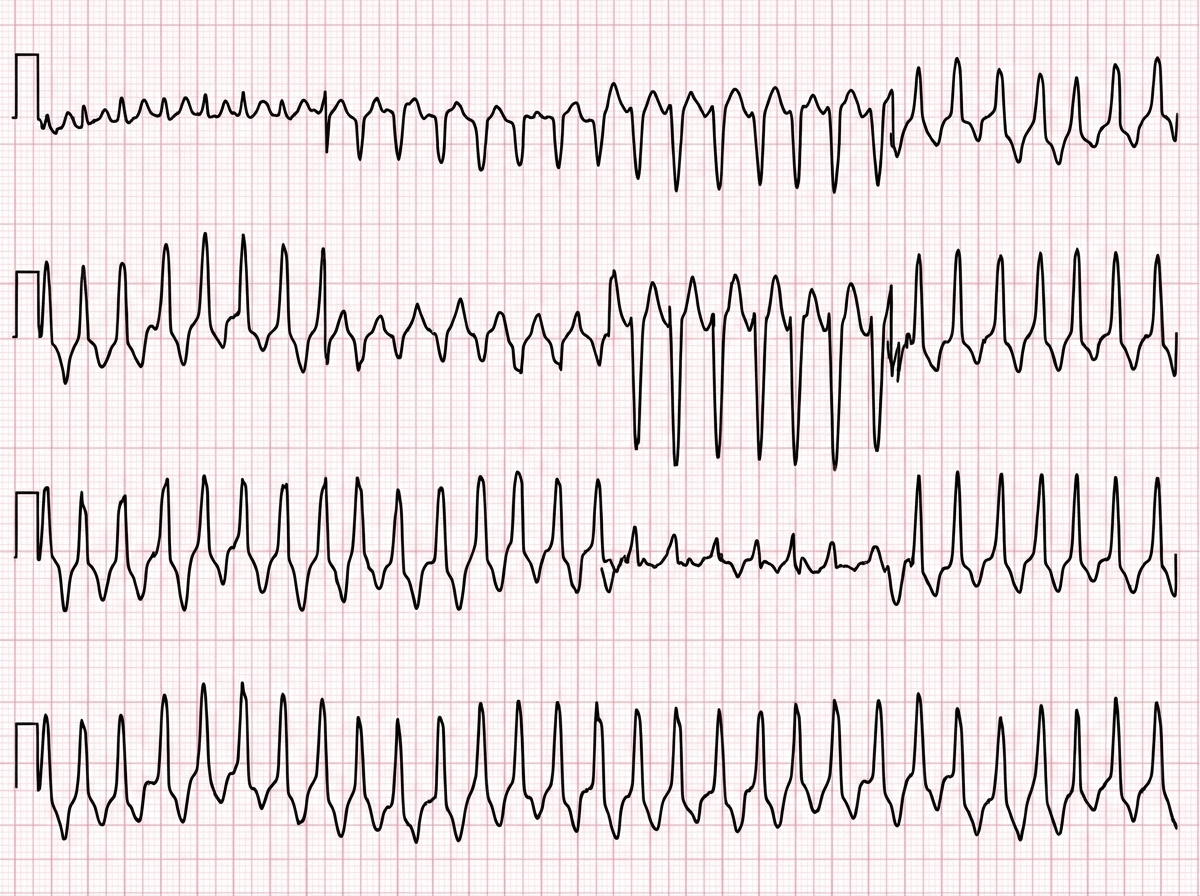
A 54-year-old man presents to the emergency department with palpitations and dizziness. He has a pulse, blood pressure is 110/70 mmHg, and he is hemodynamically stable. His QTc interval is normal. The ECG is shown below. What is the best drug for the rhythm disorder shown?
What is the best treatment for multifocal atrial tachycardia?
What percentage of critical narrowing of coronary blood vessels is generally considered significant?
Pulsus paradoxus is present in all of the following conditions EXCEPT:
A 45-year-old man presents with exertional dyspnea and pitting pedal edema. His neck veins are dilated. A diagnosis of superior vena cava (SVC) syndrome is made. What is the next diagnostic step?
Atrial myxoma is associated with which of the following clinical manifestations, except?
Left axis deviation is seen in all except?
A 22-year-old woman presents with sharp chest pain, exacerbated by lying down, especially on her left side. One week prior, she experienced flu-like symptoms with fevers, chills, and myalgias. Her past medical history is negative, and she takes no medications. On physical examination, blood pressure is 130/80 mm Hg, heart rate is 100/min, with no pulsus paradoxus. Heart sounds are normal, but a pericardial rub is heard best at the apex in the left lateral decubitus position. Lungs are clear, and there is no peripheral edema. Which of the following features determines the patient's clinical course and prognosis?
What is the most common cardiac arrhythmia?
Which of the following cardiac rhythms is NOT associated with hyperkalemia?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app