
Cardiology — MCQs

On this page
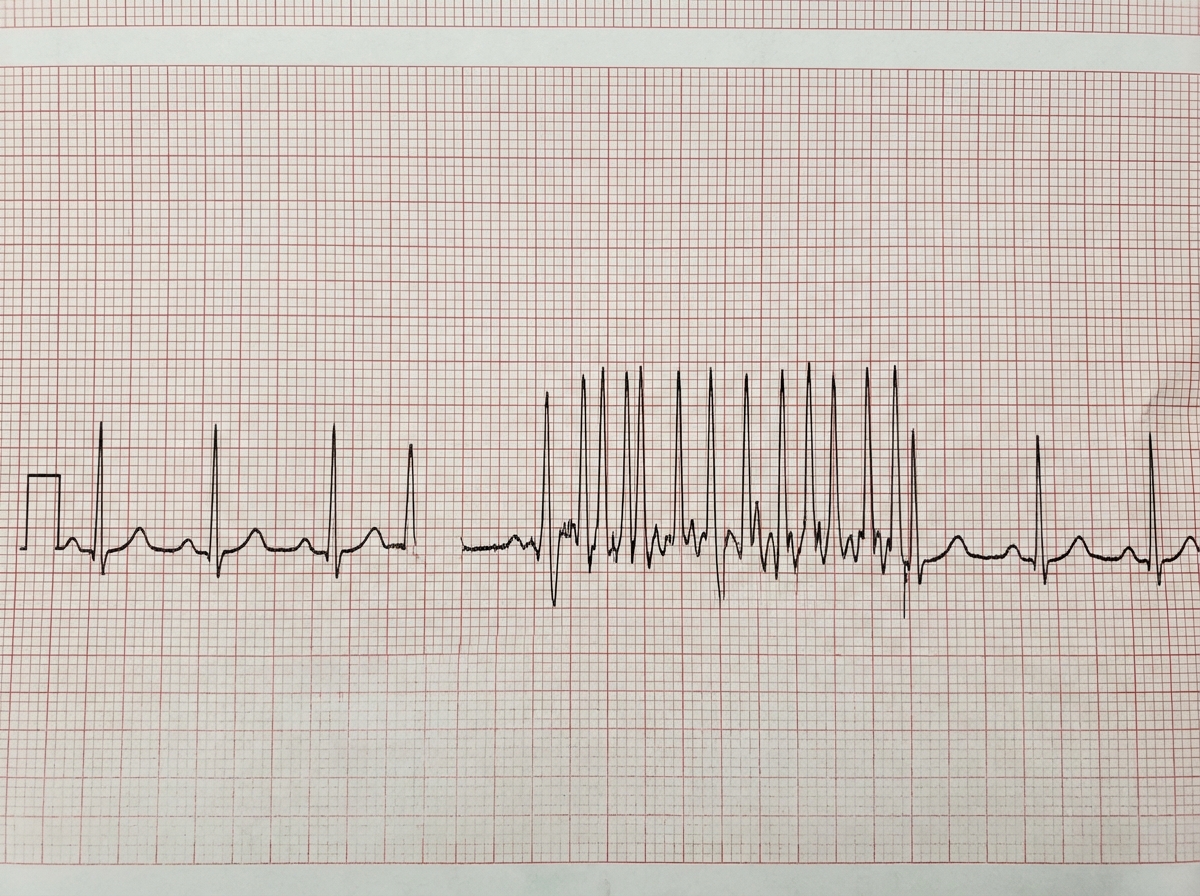
A 50-year-old patient complains of dizziness and palpitations. What does the ECG show?
Which of the following is true regarding neurocardiogenic syncope?
What is the earliest feature of pulmonary venous hypertension?
Which of the following agents should NOT be used for oral anticoagulation in high-risk patients with atrial fibrillation?
A 35-year-old athlete with a height of 184 cm, arm span of 194 cm, pulse rate of 64/min, and BP of 148/64 mm Hg presents with a long diastolic murmur heard over the right second intercostal space on routine chest auscultation. What is the probable diagnosis?
Which of the following conditions is associated with a QRS duration greater than 0.16 seconds?
Three weeks after surgery to implant a mechanical aortic valve, a 70-year-old man develops chest pain, fever, and leukocytosis. On examination, the JVP is increased, there is a mechanical S2 sound, and a pericardial friction rub. Which of the following is the most likely diagnosis?
Which of the following conditions causes a wide pulse pressure?
An 18-year-old man is admitted to the hospital with acute onset of substernal chest pain that began abruptly 30 minutes ago. The pain radiates to his neck and right arm. He has otherwise been in good health. On physical examination, he is diaphoretic and tachypnoeic. His BP is 102/48 mmHg and heart rate is 112 bpm, with a regular rhythm but is tachycardiac. A 2/6 holosystolic murmur is heard best at the apex and radiates to the axilla. His lungs have bilateral rales at the bases. The ECG demonstrates 4 mm of ST elevation in the anterior leads. In the past, he was hospitalized for some problem with his heart when he was 4 years old. His mother, who accompanies him, reports that he received aspirin and gamma globulin as treatment. Since that time, he has required intermittent follow-up with echocardiography. What is the most likely cause of this patient's acute coronary syndrome?
Which of the following findings is NOT seen in primary pulmonary hypertension?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app