
Cardiology — MCQs

On this page
What is the treatment for orthostatic hypotension?
Dressler's syndrome is due to:
What is the relationship between the S1 ejection click and severe pulmonary stenosis?
What is the initial pharmacological treatment for sinus bradycardia in the context of myocardial infarction?
Which of the following statements is TRUE in diastolic dysfunction of the left ventricle?
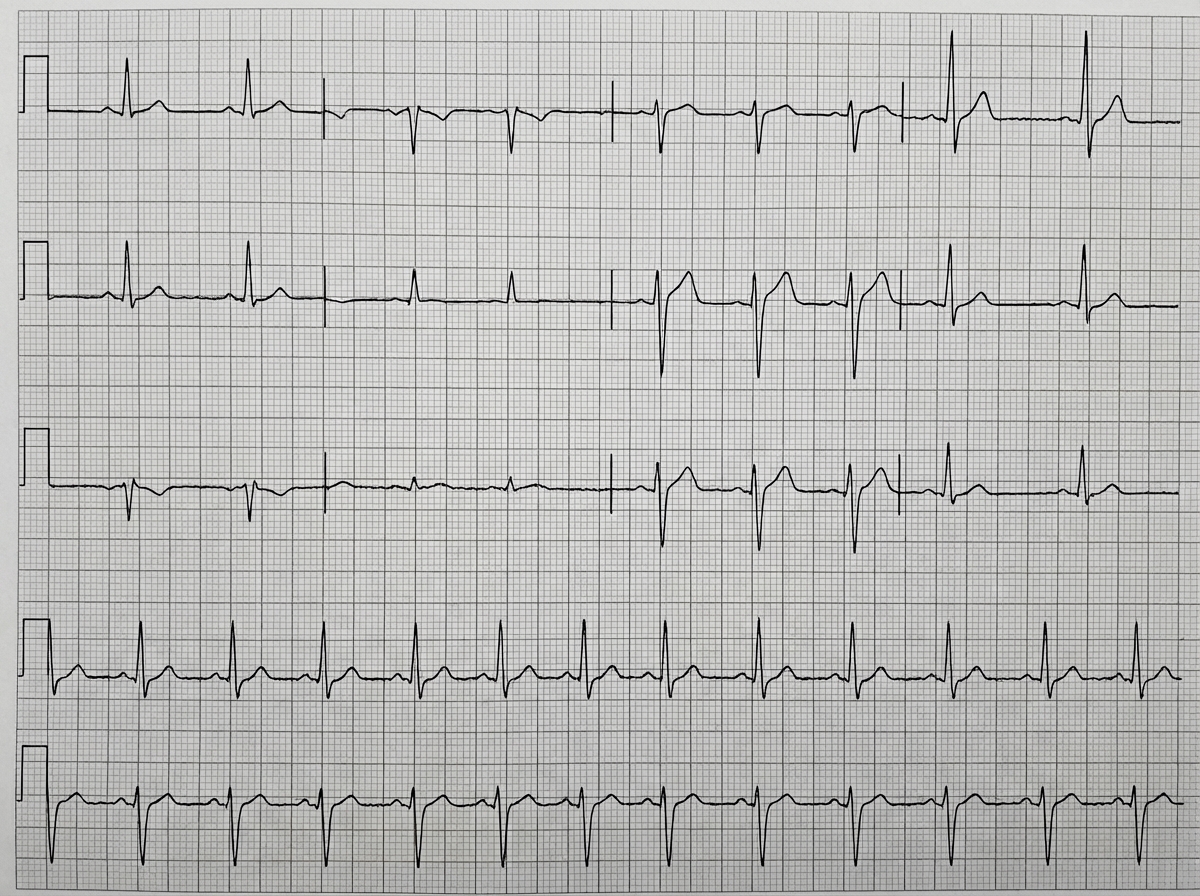
The ECG given below is seen in which condition?
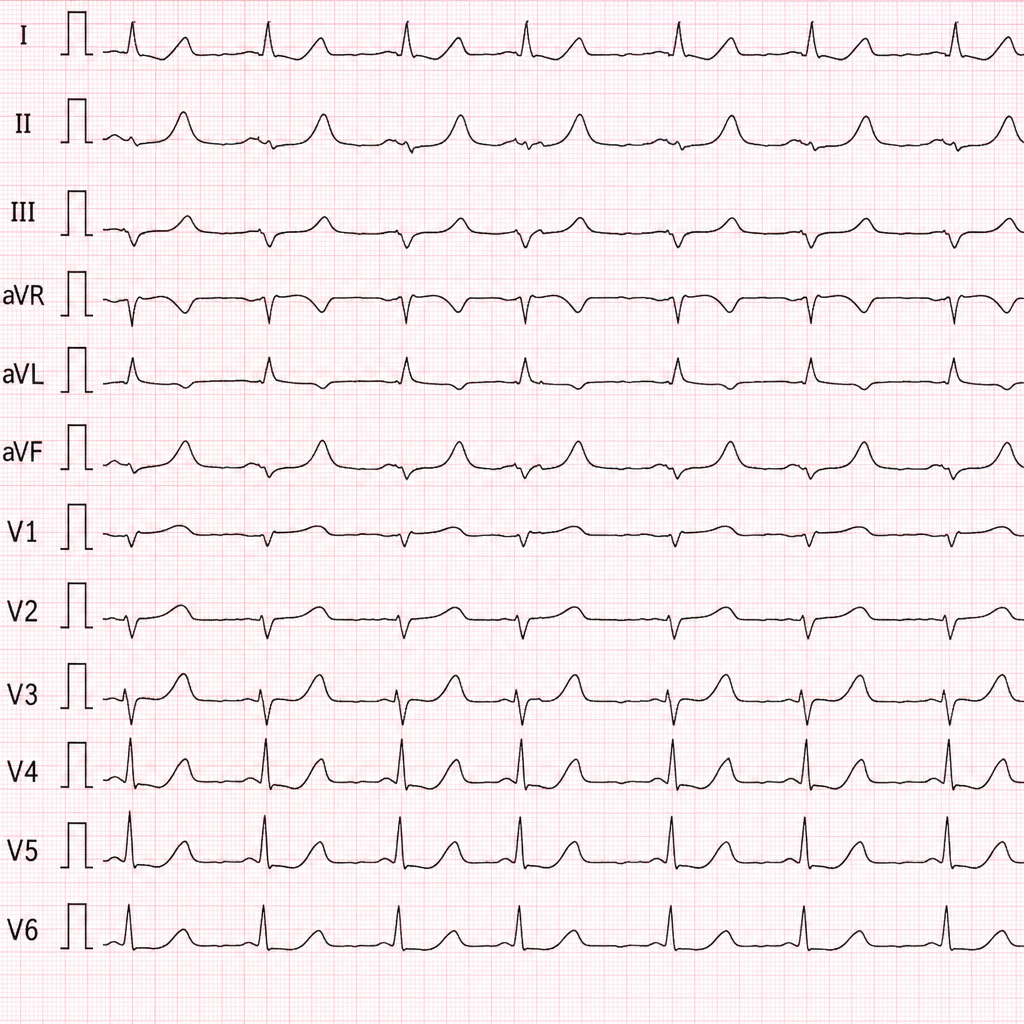
A 45-year-old man presents with central chest pain for 4 hours. Troponin I is 0.8 ng/mL (upper reference limit: 0.04 ng/mL). The ECG shows ST-segment elevation in the anterior precordial leads (V1–V4), consistent with LAD territory occlusion. What is the diagnosis?
Which type of Atrial Septal Defect (ASD) is associated with a murmur similar to Mitral Regurgitation (MR) and left axis deviation?
Which condition presents with a single second heart sound?
Which of the following drugs is MOST suitable for a 45-year old diabetic with blood pressure 150/95 mmHg?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app