
Cardiology — MCQs

On this page
True regarding atrial fibrillation?
Which condition is characterized by a 'hockey-stick' appearance on echocardiography?
Which of the following statements about blood pressure measurement is INCORRECT?
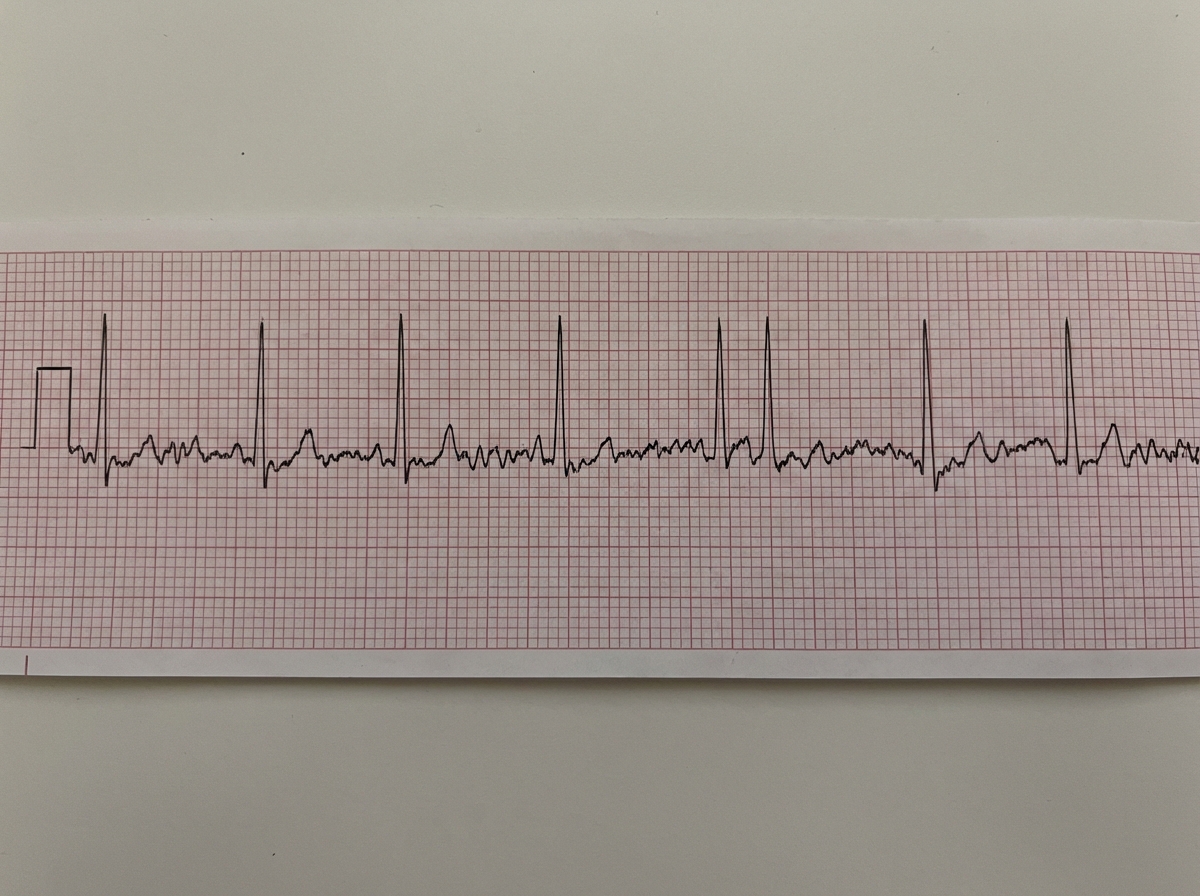
A patient in CCU on day 2 of PCI procedure has the following rhythm. BP=90/60mmHg. Which is the next best step for management of this patient?

A 56-year-old man presents with severe chest pain and difficulty in breathing. An immediate ECG was taken. What diagnosis does the ECG suggest?
Troponin-T is preferable to CPK-MB in the diagnosis of acute myocardial infarction in all of the following situations except:
A female patient presents with short stature and a history of wearing socks even in the summer season. Physical examination reveals icy cold toes with cyanosis. What is the likely underlying condition?
Which of the following arrhythmias is most likely to be heritable?
A young male with acute myeloid leukemia was treated with induction chemotherapy. Two months later, he presents with bilateral pedal edema and dyspnea on exertion, as well as paroxysmal nocturnal dyspnea. Which of the following is the most likely cause of his current symptoms?
Which of the following is not an indicator of chronic congestive heart failure?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app