
Cardiology — MCQs

On this page
A healthy middle-aged man who became emotionally upset during an argument with his brother suddenly developed chest pain and collapsed. He was declared dead upon arrival at the hospital. What is the most likely diagnosis?
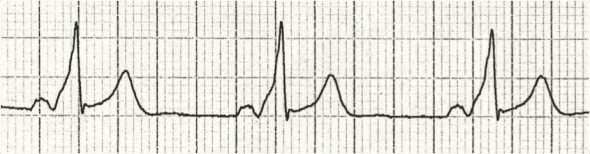
In which condition are epsilon waves observed on an ECG?
Which of the following is the most appropriate true statement regarding ostium primum atrial septal defect (ASD)?
Which is not a major criterion of Jones in rheumatic fever?
A lady presents with grade 3 dyspnea, severe mitral stenosis, and atrial fibrillation, with an increased ventricular rate and a clot in the left atrium. Which of the following should not be done?
A 4-year-old girl is brought to the pediatrician's office, where her father reports that she suddenly became pale and stopped running while playfully chasing her and her pet Chihuahua. After 30 minutes, she was no longer pale and wanted to resume the game. She has never had a previous episode and has never been cyanotic. Her physical examination was normal, as were her chest x-ray and echocardiogram. An ECG shows a specific pattern indicating which of the following?
Where are venous emboli most often lodged?
Straight back syndrome is associated with?
Which of the following is a characteristic feature of Takayasu arteritis?
A 38-year-old man presents with pain and shortness of breath. His pulse rate is 85 per minute, blood pressure is 180/80 mmHg, and the cardiac examination reveals an ejection systolic murmur. The ECG shows a LVH pattern and ST depression in the anterior leads. His Troponin T test is positive. Based on these findings, the echocardiogram is likely to reveal which of the following conditions?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app