
Cardiology — MCQs

On this page
A 30-year-old man presents with cramping gluteal pain after walking 500m. Which vascular condition is most likely involved?
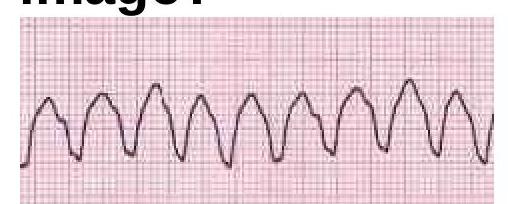
Identify the cardiac condition represented in the image.
Which type of cardiomyopathy is associated with alcohol abuse?
What does the CEAP score classify?
In which of the following conditions is the implantation of an Automatic Implantable Cardioverter Defibrillator (AICD) indicated?
In which condition does the Ankle-Brachial Pressure Index (ABPI) increase artificially?
What are the potential causes of cardiogenic shock excluding myocardial infarction?
What electrolyte imbalance is most commonly associated with prominent U waves on ECG?
Roth spots are associated with which of the following conditions?
Which drug is used as an adjunct to epinephrine in refractory ventricular fibrillation/ventricular tachycardia during cardiac arrest?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app