
Cardiology — MCQs

On this page
What is the preferred treatment for a patient diagnosed with acute pericarditis?
A 72-year-old female with atrial fibrillation on warfarin presents with sudden severe abdominal pain. Examination reveals a distended abdomen and decreased bowel sounds. Laboratory results show an INR of 4.5 and hemoglobin of 9.1. Analyze and determine the diagnosis and initial treatment.
A 45-year-old man presents with exertional dyspnea and swelling of his legs. An echocardiogram shows left ventricular hypertrophy and systolic dysfunction. What is the most likely underlying cause?
Which medication is indicated for the long-term management of patients with stable ischemic heart disease to reduce the risk of myocardial infarction?
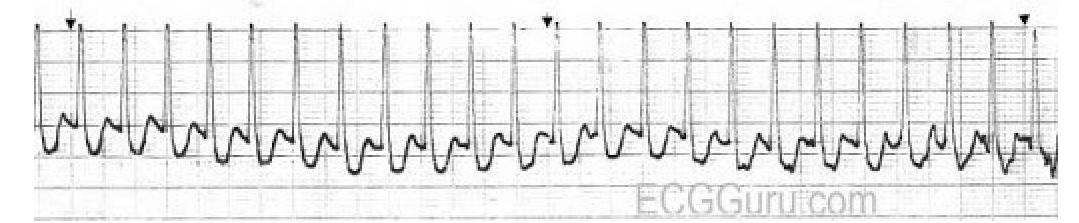
Identify the diagnosis based on the provided ECG image.
Which murmur increases on standing?
Most characteristic cardiovascular defect seen in Rubella-
A patient presents with chest pain and an ECG showing ST-segment elevation. After treatment, the ECG shows resolution of ST-segment changes, but the patient continues to have chest pain. What is the most likely diagnosis?
What is a potential cause of cardiogenic shock other than myocardial infarction (MI)?
In ACLS, which drug is recommended for use after unsuccessful defibrillation attempts following ventricular fibrillation?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app